

Antimicrobial Resistance Trends in Urine Escherichia coli Isolates From Adult and Adolescent Females in the United States From 2011 to 2019: Rising ESBL Strains and Impact on Patient Management
- PMID: 34143881
- PMCID: PMC8664433
- DOI: 10.1093/cid/ciab560
Antimicrobial Resistance Trends in Urine Escherichia coli Isolates From Adult and Adolescent Females in the United States From 2011 to 2019: Rising ESBL Strains and Impact on Patient Management
Abstract
Background: Uncomplicated urinary tract infection (uUTI) is predominantly caused by Escherichia coli, which has increasing antimicrobial resistance (AMR) at the United States (US)-community level. As uUTI is often treated empirically, assessing AMR is challenging, and there are limited contemporary data characterizing period prevalence in the US.
Methods: This was a retrospective study of AMR using Becton, Dickinson and Company Insights Research Database (Franklin Lakes, New Jersey, US) data collected 2011-2019. Thirty-day, nonduplicate Escherichia coli urine isolates from US female outpatients (aged ≥12 years) were included. Isolates were evaluated for nonsusceptibility (intermediate/resistant) to trimethoprim-sulfamethoxazole, fluoroquinolones, or nitrofurantoin, and assessed for extended-spectrum β-lactamase production (ESBL+) and for ≥2 or ≥3 drug-resistance phenotypes. Generalized estimating equations were used to model AMR trends over time and by US census region.
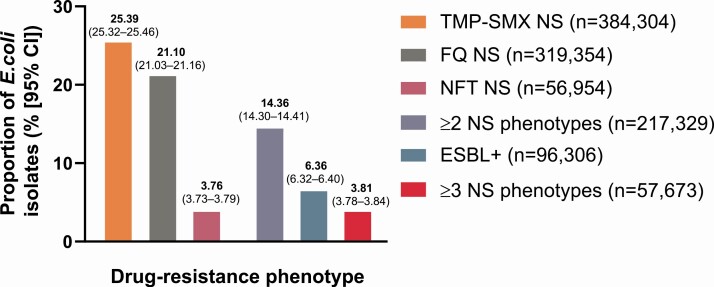
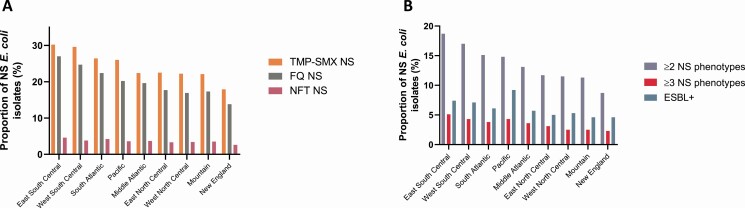
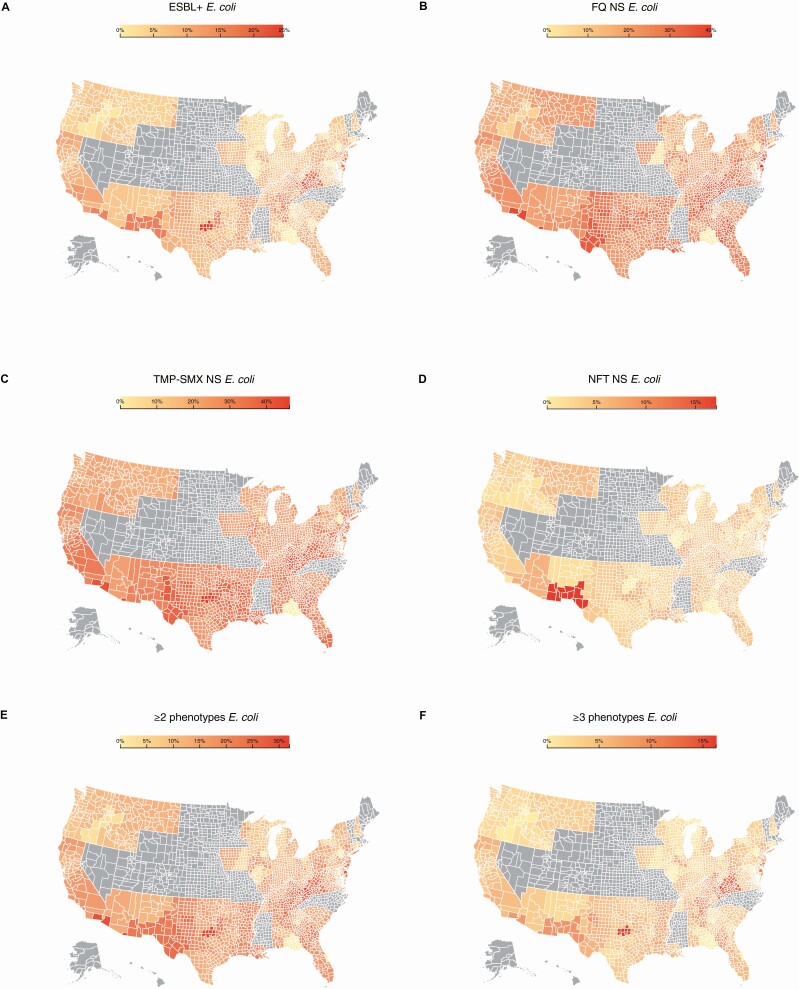
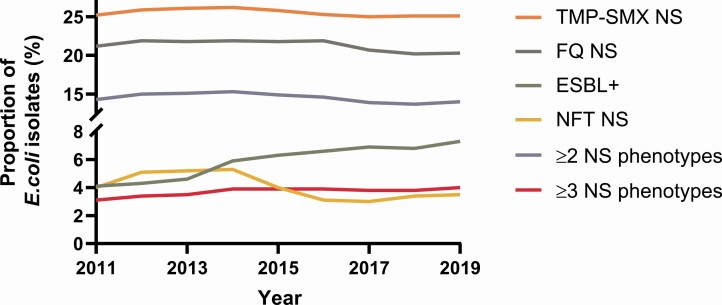
Results: Among 1 513 882 E. coli isolates, the overall prevalence of isolates nonsusceptible to trimethoprim-sulfamethoxazole, fluoroquinolones, and nitrofurantoin was 25.4%, 21.1%, and 3.8%, respectively. Among the isolates, 6.4% were ESBL+, 14.4% had ≥2 drug-resistance phenotypes, and 3.8% had ≥3. Modeling demonstrated a relative average yearly increase of 7.7% (95% confidence interval [CI], 7.2-8.2%) for ESBL+ isolates and 2.7% (95% CI, 2.2-3.2%) for ≥3 drug-phenotypes (both P < .0001). Modeling also demonstrated significant variation in AMR prevalence between US census regions (P < .001).
Conclusions: Period prevalence of AMR among US outpatient urine-isolated E. coli was high, and for multidrug-resistance phenotypes increased during the study period with significant variation between census regions. Knowledge of regional AMR rates helps inform empiric treatment of community-onset uUTI and highlights the AMR burden to physicians.
Keywords: Escherichia coli; antimicrobial resistance; antimicrobial stewardship; uncomplicated urinary tract infection.
© The Author(s) 2021. Published by Oxford University Press for the Infectious Diseases Society of America.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
