

ATP and adenosine-Two players in the control of seizures and epilepsy development
- PMID: 34144123
- PMCID: PMC10237002
- DOI: 10.1016/j.pneurobio.2021.102105
ATP and adenosine-Two players in the control of seizures and epilepsy development
Abstract
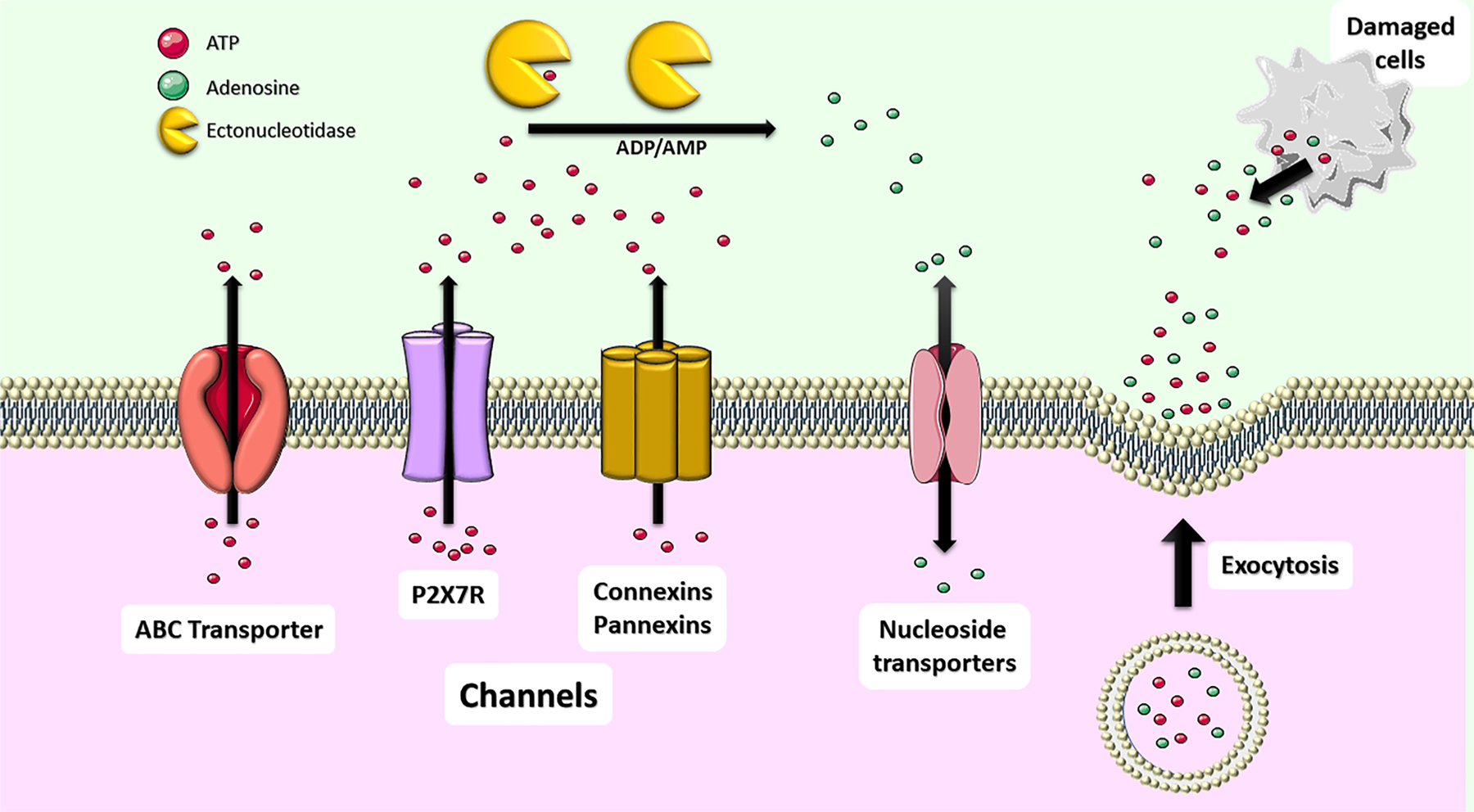
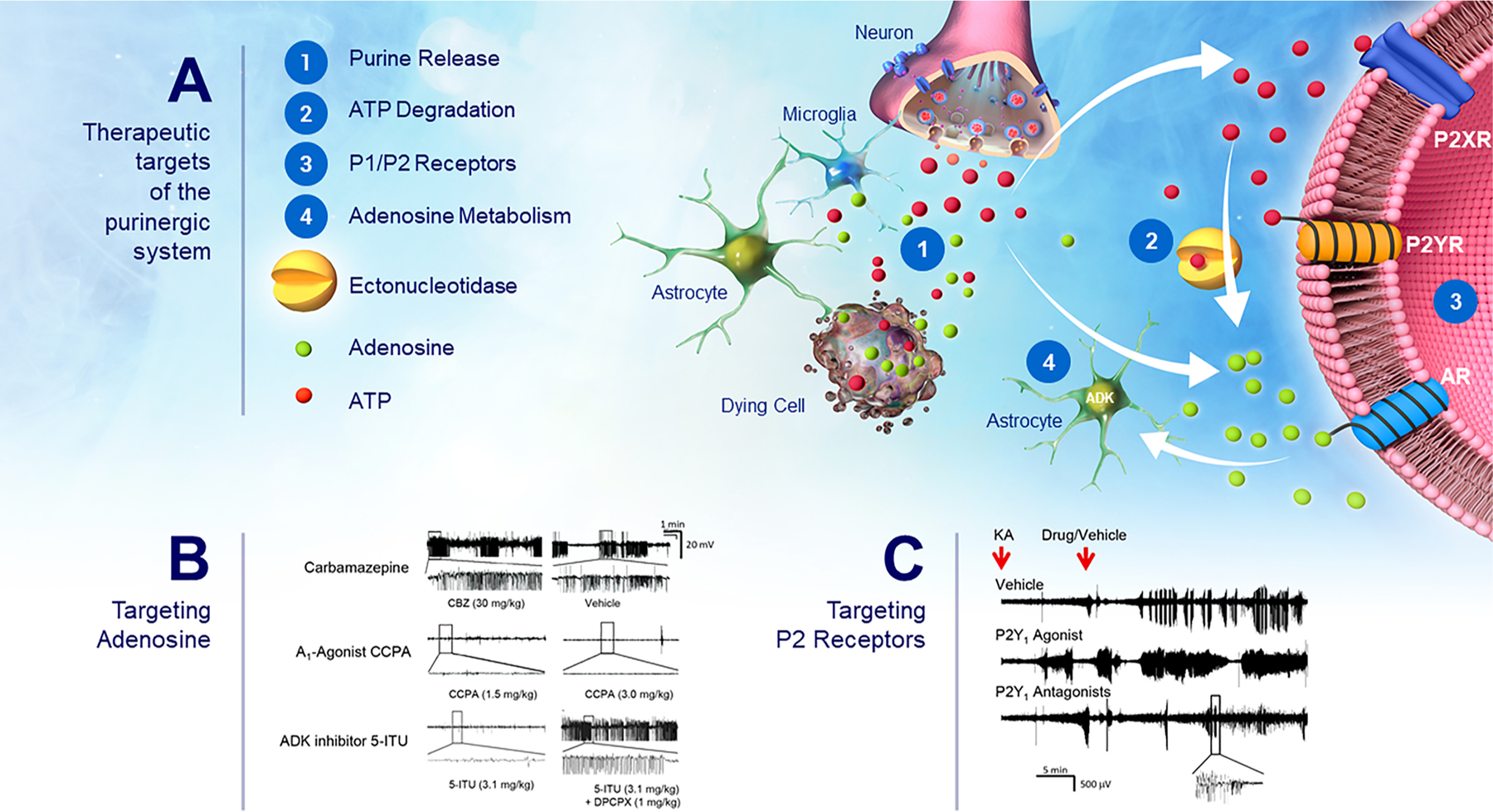
Despite continuous advances in understanding the underlying pathogenesis of hyperexcitable networks and lowered seizure thresholds, the treatment of epilepsy remains a clinical challenge. Over one third of patients remain resistant to current pharmacological interventions. Moreover, even when effective in suppressing seizures, current medications are merely symptomatic without significantly altering the course of the disease. Much effort is therefore invested in identifying new treatments with novel mechanisms of action, effective in drug-refractory epilepsy patients, and with the potential to modify disease progression. Compelling evidence has demonstrated that the purines, ATP and adenosine, are key mediators of the epileptogenic process. Extracellular ATP concentrations increase dramatically under pathological conditions, where it functions as a ligand at a host of purinergic receptors. ATP, however, also forms a substrate pool for the production of adenosine, via the action of an array of extracellular ATP degrading enzymes. ATP and adenosine have assumed largely opposite roles in coupling neuronal excitability to energy homeostasis in the brain. This review integrates and critically discusses novel findings regarding how ATP and adenosine control seizures and the development of epilepsy. This includes purine receptor P1 and P2-dependent mechanisms, release and reuptake mechanisms, extracellular and intracellular purine metabolism, and emerging receptor-independent effects of purines. Finally, possible purine-based therapeutic strategies for seizure suppression and disease modification are discussed.
Keywords: Adenosine; Adenosine triphosphate; Epilepsy; P1 receptors; P2 receptors; Purinergic signaling.
Copyright © 2021 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Figures

References
-
- Adami M, Bertorelli R, Ferri N, Foddi MC, Ongini E, 1995. “Effects of repeated administration of selective adenosine A1 and A2A receptor agonists on pentylenetetrazole-induced convulsions in the rat.”. Eur. J. Pharmacol 294 (2–3), 383–389. - PubMed
-
- Adinolfi E, Giuliani AL, De Marchi E, Pegoraro A, Orioli E, Di Virgilio F, 2018. “The P2X7 receptor: a main player in inflammation.”. Biochem. Pharmacol 151, 234–244. - PubMed
-
- Alves M, Gomez-Villafuertes R, Delanty N, Farrell MA, O’Brien DF, Miras-Portugal MT, Hernandez MD, Henshall DC, Engel T, 2017. “Expression and function of the metabotropic purinergic P2Y receptor family in experimental seizure models and patients with drug-refractory epilepsy.”. Epilepsia 58 (9), 1603–1614. - PubMed
