

Postural orthostatic tachycardia syndrome (POTS): State of the science and clinical care from a 2019 National Institutes of Health Expert Consensus Meeting - Part 1
- PMID: 34144933
- PMCID: PMC8455420
- DOI: 10.1016/j.autneu.2021.102828
Postural orthostatic tachycardia syndrome (POTS): State of the science and clinical care from a 2019 National Institutes of Health Expert Consensus Meeting - Part 1
Abstract
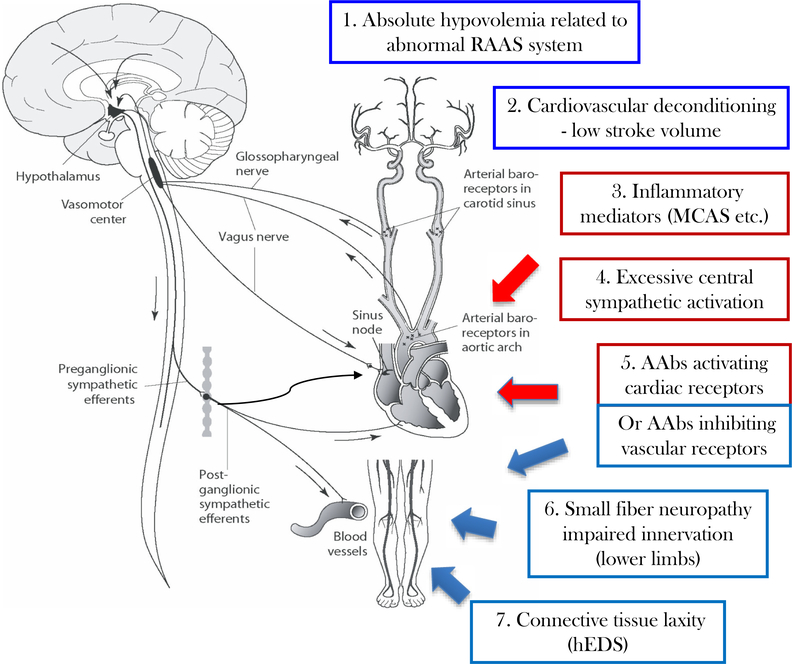
Postural orthostatic tachycardia syndrome (POTS) is a chronic and often disabling disorder characterized by orthostatic intolerance with excessive heart rate increase without hypotension during upright posture. Patients often experience a constellation of other typical symptoms including fatigue, exercise intolerance and gastrointestinal distress. A typical patient with POTS is a female of child-bearing age, who often first displays symptoms in adolescence. The onset of POTS may be precipitated by immunological stressors such as a viral infection. A variety of pathophysiologies are involved in the abnormal postural tachycardia response; however, the pathophysiology of the syndrome is incompletely understood and undoubtedly multifaceted. Clinicians and researchers focused on POTS convened at the National Institutes of Health in July 2019 to discuss the current state of understanding of the pathophysiology of POTS and to identify priorities for POTS research. This article, the first of two articles summarizing the information discussed at this meeting, summarizes the current understanding of this disorder and best practices for clinical care. The evaluation of a patient with suspected POTS should seek to establish the diagnosis, identify co-morbid conditions, and exclude conditions that could cause or mimic the syndrome. Once diagnosed, management typically begins with patient education and non-pharmacologic treatment options. Various medications are often used to address specific symptoms, but there are currently no FDA-approved medications for the treatment of POTS, and evidence for many of the medications used to treat POTS is not robust.
Keywords: Expert consensus; Pathophysiology; Postural orthostatic tachycardia syndrome; Treatment; Workshop.
Copyright © 2021 The Authors. Published by Elsevier B.V. All rights reserved.
Figures
References
-
- Abe H, Nagatomo T, Kohshi K, Numata T, Kikuchi K, Sonoda S, Mizuki T, Kuroiwa A, Nakashima Y, 2000. Heart rate and plasma cyclic AMP responses to isoproterenol infusion and effect of beta-adrenergic blockade in patients with postural orthostatic tachycardia syndrome. J. Cardiovasc. Pharmacol. 36 (Suppl. 2), S79–S82. 10.1097/00005344-200000006-00017. - DOI - PubMed
-
- Barcroft H, Edholm OG, McMichael J, Sharpey-Shafer EP, 1944. Posthaemorrhagic fainting: study by cardiac output and forearm flow. Lancet 1, 489–491.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
