

KarMMa-RW: comparison of idecabtagene vicleucel with real-world outcomes in relapsed and refractory multiple myeloma
- PMID: 34145225
- PMCID: PMC8213772
- DOI: 10.1038/s41408-021-00507-2
KarMMa-RW: comparison of idecabtagene vicleucel with real-world outcomes in relapsed and refractory multiple myeloma
Abstract
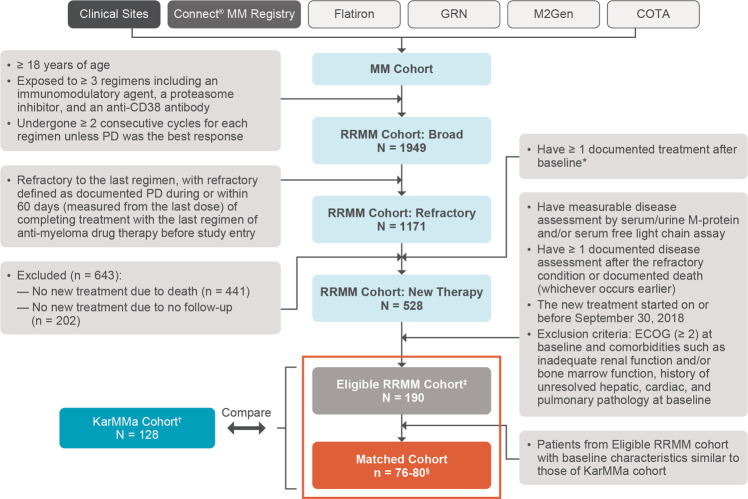
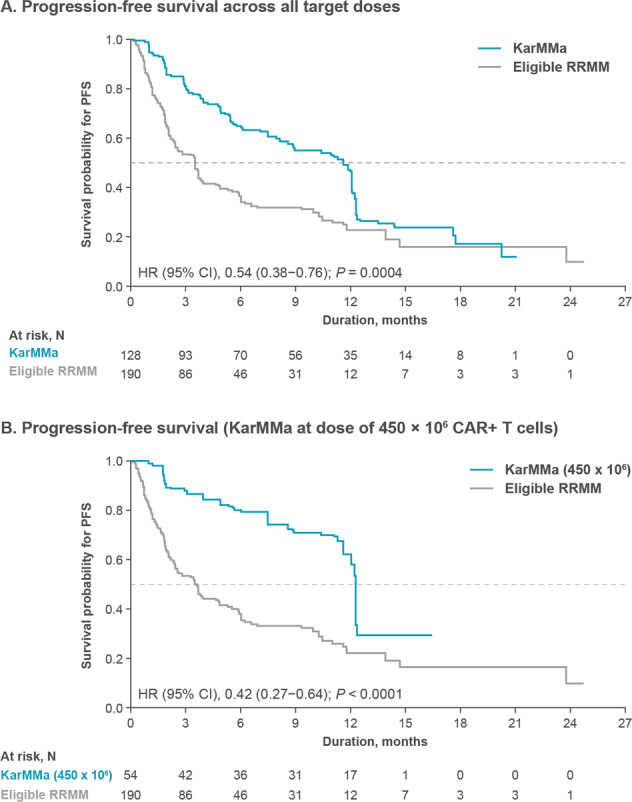
Patients with relapsed and refractory multiple myeloma (RRMM) who are triple-class exposed (to an immunomodulatory agent, proteasome inhibitor, and anti-CD38 antibody) have limited treatment options and there is no standard of care. Idecabtagene vicleucel (ide-cel, bb2121), a BCMA-directed CAR T-cell therapy, demonstrated efficacy in triple-class exposed RRMM patients in the KarMMa trial (NCT03361748). In this retrospective study (KarMMa-RW), patient-level data from triple-class exposed RRMM patients were merged into a single data model and compared with KarMMa using trimmed stabilized inverse probability of treatment weighting. Endpoints included overall response rate (ORR; primary), rate of very good partial response or better (≥VGPR), progression-free survival (PFS), and overall survival (OS). Of 1949 real-world triple-class exposed RRMM patients, 190 received subsequent (index) line of therapy and met KarMMa eligibility criteria (Eligible RRMM cohort). With a median follow-up of 13.3 months in KarMMa and 10.2 months in Eligible RRMM, ORR, and ≥VGPR were significantly improved in KarMMa versus Eligible RRMM (ORR, 76.4% vs 32.2%; ≥VGPR, 57.9% vs 13.7%; both P < 0.0001) as were PFS (11.6 vs 3.5 months; P = 0.0004) and OS (20.2 vs 14.7 months; P = 0.0006). This study demonstrated that ide-cel significantly improved responses and survival compared with currently available therapies in triple-class exposed RRMM.
Conflict of interest statement
S.J. served as a consultant for Bristol Myers Squibb (BMS), Janssen, Legend Biotech, Sanofi, and Takeda. Y.L. served as a consultant for Kite/Gilead, Celgene (a BMS Company), Juno Therapeutics (a BMS Company), bluebird bio, Janssen, Legend Biotech, Gamida Cells, and Novartis; received research funding from Kite/Gilead, Celgene (a BMS Company), bluebird bio, Janssen, Merck, and Takeda; is a member of Sorrento Therapeutics Data and Safety Monitoring Board. H.G. received grants and/or provision of investigational medicinal product from Amgen, BMS, Celgene (a BMS Company), Chugai, Dietmar-Hopp-Foundation, Janssen, Johns Hopkins University, and Sanofi; received research funding from Amgen, BMS, Celgene (a BMS Company), Chugai, Janssen, Incyte, Molecular Partners, Merck, Sharp and Dohme, Sanofi, Mundipharma, Takeda, and Novartis; served as a member of advisory board for Adaptive Biotechnologies, Amgen, BMS, Janssen, Sanofi, and Takeda; participated in the speakers’ bureau for Amgen, BMS, Celgene (a BMS Company), Chugai, GlaxoSmithKline (GSK), Janssen, Novartis, and Sanofi. D.R. served as a consultant for Celgene (a BMS Company), Janssen, Takeda, Amgen, and Karyopharm; received honoraria from Celgene (a BMS Company), Janssen, Takeda, and Amgen; received research funding from Celgene (a BMS Company), Janssen, Takeda, Otsuka, Merck, and BMS; provided expert testimony for Celgene (a BMS Company) and Amgen. A.N. served as a consultant for Spectrum Pharmaceuticals, BMS, Adaptive Biotechnologies, Amgen, Celgene (a BMS Company), Takeda, Karyopharm, Oncopeptides, GSK, and Janssen; received research funding from BMS, Amgen, Celgene (a BMS Company), Takeda, Karyopharm, GSK, and Janssen. P.R.O. served as a consultant for Celgene (a BMS Company), Janssen, AbbVie, Kite Pharma, and Sanofi; participated in the speakers’ bureau for Celgene (a BMS Company), Janssen, and Amgen; received travel funding from Celgene (a BMS Company). K.M. received honoraria from Celgene (a BMS Company), Takeda, and Janssen. N.S. served as a consultant for Genentech, Seagen Inc., Oncopeptides, Karyopharm, Surface Oncology, Precision Biosciences, GSK, Nektar, Amgen, Indapta Therapeutics, Sanofi, and BMS; received research funding from Celgene (a BMS Company), Janssen, bluebird bio, Sutro Biopharma, and Teneobio. L.D.A. served as a consultant for Amgen, BMS, GSK, Janssen, and Karyopharm; received research funding and honoraria from GSK, BMS, Janssen, Karyopharm, and Amgen. K.W., H.V.L., A.A. are employees and equity owners with BMS. A.S.S. was an employee of BMS at the time the work was completed. D.S.S. served as a consultant for Amgen, Celgene (a BMS Company), Takeda, Janssen, BMS, Karyopharm, and Merck; participated in the speakers’ bureau for Amgen, Celgene (a BMS Company), Takeda, Janssen, and BMS; received research funding from Celgene (a BMS Company); is an equity owner with Celularity. A.S., R.P., and M.S. declare no conflict of interest.
Figures


References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
