

Multi-omics profiling of primary small cell carcinoma of the esophagus reveals RB1 disruption and additional molecular subtypes
- PMID: 34145257
- PMCID: PMC8213753
- DOI: 10.1038/s41467-021-24043-6
Multi-omics profiling of primary small cell carcinoma of the esophagus reveals RB1 disruption and additional molecular subtypes
Abstract
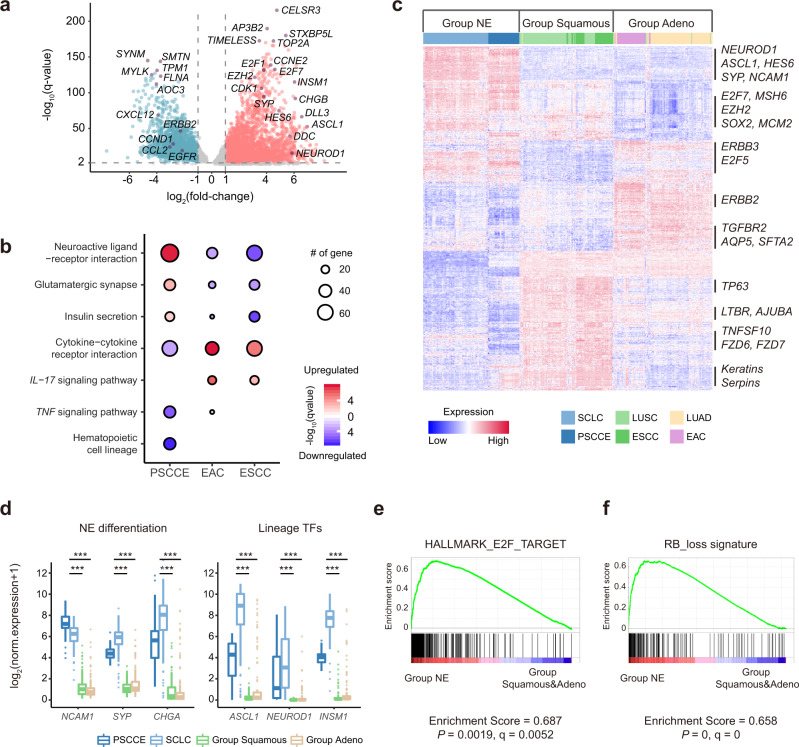
Primary small cell carcinoma of the esophagus (PSCCE) is a lethal neuroendocrine carcinoma. Previous studies proposed a genetic similarity between PSCCE and esophageal squamous cell carcinoma (ESCC) but provided little evidence for differences in clinical course and neuroendocrine differentiation. We perform whole-exome sequencing, RNA sequencing and immunohistochemistry profiling on 46 PSCCE cases. Integrated analyses enable the discovery of multiple mechanisms of RB1 disruption in 98% (45/46) of cases. The transcriptomic landscape of PSCCE closely resembles small cell lung cancer (SCLC) but differs from ESCC or esophageal adenocarcinoma (EAC). Distinct gene expression patterns regulated by ASCL1 and NEUROD1 define two molecular subtypes, PSCCE-A and PSCCE-N, which are highly similar to SCLC subtypes. A T cell excluded phenotype is widely observed in PSCCE. In conclusion, PSCCE has genomic alterations, transcriptome features and molecular subtyping highly similar to SCLC but distinct from ESCC or EAC. These observations are relevant to oncogenesis mechanisms and therapeutic vulnerability.
Conflict of interest statement
The authors declare no competing interests.
Figures





References
-
- Patel S, TenNapel M, Clamon G, Bhatia S. Small cell carcinoma of the esophagus: the SEER experience from 2000–2009. Int. J. Radiat. Oncol.*Biol.*Phys. 2013;87:S292. doi: 10.1016/j.ijrobp.2013.06.766. - DOI
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
