

[Thyroid function of first-trimester twin pregnant women and its association with preterm delivery]
- PMID: 34145847
- PMCID: PMC8220037
- DOI: 10.19723/j.issn.1671-167X.2021.03.006
[Thyroid function of first-trimester twin pregnant women and its association with preterm delivery]
Abstract
Objective: To describe the thyroid function abnormality of first-trimester twin pregnant women according to different references, and to explore its association with preterm delivery.
Methods: Participants, first-trimester twin pregnant women, were recruited at Peking University Third Hospital from March 2017 to February 2020. The thyroid hormone reference for ordinary adults identified on the assay kits by Siemens incorporation, thyroid hormone reference specifically for singleton pregnancy established previously, and thyroid hormone reference specifically for twin pregnancy established previously were used in the description of hypothyroidism and hyperthyroidism for first-trimester twin pregnant women. Thyroid autoantibody reference identified on the assay kits by Siemens incorporation was used in the description of positive thyroid autoantibody. Multivariable log-binomial regression was conducted to examine the association between thyroid function and preterm delivery, in which normal pregnant women according to the three references and normal pregnant women according to twin pregnancy reference accompanied with negative thyroid autoantibody were taken as control respectively.
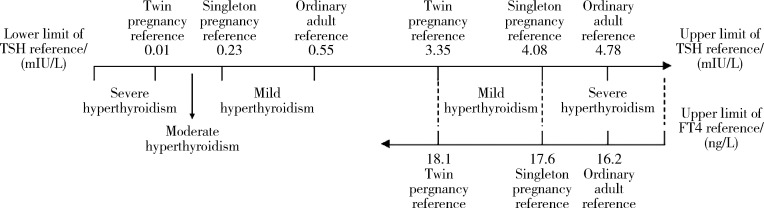
Results: A total of 570 twin pregnant women were finally included. Rates of hypothyroidism according to the three references were 1.2%, 1.6% and 3.5%, respectively. Rates of hyperthyroidism according to the three references were 32.6%, 18.1% and 1.1%, respectively. After adjustment for potential confounding factors, risk of preterm delivery significantly increased in pregnant women with hyperthyroidism according to the twin specific pregnancy reference [adjusted relative risk (ARR)=1.41, 95%CI: 1.14-1.75], while no significant increase was found in those with normal thyroid function according to the twin specific pregnancy reference but hyperthyroidism according to the singleton specific pregnancy reference (ARR=1.00, 95%CI: 0.81-1.25) and in those with hyperthyroidism purely according to the ordinary adult reference (ARR=1.06, 95%CI: 0.85-1.32), compared with those normal according to all the references. Risks of preterm delivery almost significantly or significantly increased in pregnant women with hypothyroidism according to the ordinary adult or singleton specific pregnancy reference (ARR=1.40, 95%CI: 0.88-2.22) and those with hypothyroidism according to the twin specific pregnancy reference (ARR=1.53, 95%CI: 1.03-2.28). Overall analysis of thyroid function according to the twin specific pregnancy reference and thyroid autoantibody showed that risks of preterm delivery almost significantly or significantly increased in pregnant women with simple hypothyroidism (ARR=1.46, 95%CI: 0.93-2.27), simple positive thyroid autoantibody (ARR=1.32, 95%CI: 1.15-1.52), and hypothyroidism accompanied with positive thyroid autoantibody (ARR=1.78, 95%CI: 1.30-2.44), compared with those normal according to the twin specific pregnancy reference with negative thyroid autoantibody.
Conclusion: The ordinary adult reference and that of singleton pregnancy may lead to under-diagnosis of hypothyroidism and over-diagnosis of hyperthyroidism in first-trimester twin pregnant women. Compared with pregnant women with normal thyroid function, those missed in the diagnosis of hypothyroidism were at a higher risk of preterm delivery, while those over-diagnosed as hyperthyroidism had a similar risk of preterm delivery, indicating a need to develop and generalize twin-pregnancy-specific reference on common indicators of thyroid function. Moreover, the thyroid autoantibody should be taken into consideration in the prenatal diagnosis and treatment to twin pregnant women with hypothyroidism.
目的: 根据不同参考范围,描述双胎妊娠孕妇孕早期甲状腺功能异常情况,并探究其与早产的关联性。
方法: 以2017年3月至2020年2月在北京大学第三医院募集的双胎妊娠孕妇为对象,根据Siemens公司生产的检测试剂盒标识的普通成人甲状腺激素参考范围、既往研究建立的单胎妊娠特异甲状腺激素参考范围和双胎妊娠特异甲状腺激素参考范围,描述孕妇甲状腺功能减退(简称“甲减”)和甲状腺功能亢进(简称“甲亢”)情况; 根据Siemens公司生产的甲状腺自身抗体检测试剂盒标识的参考范围,描述孕妇甲状腺自身抗体阳性情况; 先后以所有参考范围均判定正常的孕妇、双胎特异参考范围判定正常且甲状腺自身抗体阴性的孕妇为对照,采用多变量对数二项式模型分析甲状腺功能与早产的关联性。
结果: 共纳入双胎妊娠孕妇570例,根据普通成人、单胎和双胎参考范围的甲减检出率依次为1.2%、1.6%和3.5%,甲亢检出率依次为32.6%、18.1%和1.1%。调整潜在混杂因素后,与根据三种参考范围判定均正常的孕妇相比,根据双胎特异参考范围判定为甲亢者的早产发生风险显著增加[调整相对危险度(adjusted relative risk,ARR)为1.41,95%置信区间(confidence interval,CI)为1.14~1.75],根据双胎特异参考范围判定为正常但根据单胎特异参考范围判定为甲亢者(ARR=1.00,95%CI: 0.81~1.25)和仅根据普通成人参考范围判定为甲亢者(ARR=1.06,95%CI: 0.85~1.32)的早产发生风险均未见显著增加; 根据普通成人或单胎特异参考范围判定为甲减者(ARR=1.40,95%CI: 0.88~2.22)和仅根据双胎特异参考范围判定为甲减者(ARR=1.53,95%CI: 1.03~2.28)的早产发生风险均临界显著或显著增加。综合双胎特异参考范围判定
结果: 与甲状腺自身抗体情况进一步分析发现,与双胎特异参考范围判定为正常且甲状腺自身抗体阴性者相比,单纯甲减者、单纯抗体阳性者以及甲减合并抗体阳性者的早产发生风险均临界显著或显著增加,ARR依次为1.46(95%CI: 0.93~2.27)、1.32(95%CI: 1.15~1.52)和1.78(95%CI: 1.30~2.44)。
结论: 根据普通成人或单胎特异参考范围判定双胎妊娠孕妇孕早期甲状腺功能可能会漏诊甲减、误诊甲亢,甲减漏诊孕妇早产发生风险高于甲状腺功能正常孕妇,甲亢误诊孕妇早产发生风险与甲状腺功能正常孕妇相仿,表明亟待建立与推广双胎妊娠特异性甲状腺功能指标参考范围; 此外,对双胎妊娠甲减孕妇进行产前诊断和治疗时还应考虑甲状腺自身抗体情况。
Keywords: Preterm delivery; Thyroid function; Twin pregnancy.
Figures
Similar articles
-
The late vanishing of a co-twin contributes to adverse perinatal outcomes in the surviving singleton.Hum Reprod. 2020 Jul 1;35(7):1553-1561. doi: 10.1093/humrep/deaa120. Hum Reprod. 2020. PMID: 32613233
-
First trimester thyroid stimulating hormone as an independent risk factor for adverse pregnancy outcome.J Matern Fetal Neonatal Med. 2017 Sep;30(18):2174-2178. doi: 10.1080/14767058.2016.1242123. Epub 2016 Oct 17. J Matern Fetal Neonatal Med. 2017. PMID: 27677438
-
Impact of maternal thyroid hormone in late pregnancy on adverse birth outcomes: A retrospective cohort study in China.Endocr J. 2021 Mar 28;68(3):317-328. doi: 10.1507/endocrj.EJ20-0377. Epub 2020 Oct 27. Endocr J. 2021. PMID: 33115985
-
Effect of levothyroxine supplementation on pregnancy loss and preterm birth in women with subclinical hypothyroidism and thyroid autoimmunity: a systematic review and meta-analysis.Hum Reprod Update. 2019 May 1;25(3):344-361. doi: 10.1093/humupd/dmz003. Hum Reprod Update. 2019. PMID: 30951172
-
Thyroid disorders in pregnancy.Nat Rev Endocrinol. 2012 Nov;8(11):650-8. doi: 10.1038/nrendo.2012.171. Epub 2012 Sep 25. Nat Rev Endocrinol. 2012. PMID: 23007317 Review.
References
-
- 《妊娠和产后甲状腺疾病诊治指南》(第2版)编撰委员会, 中华医学会内分泌学分会, 中华医学会围产医学分会 妊娠和产后甲状腺疾病诊治指南(第2版) 中华内分泌代谢杂志. 2019;35(8):636–665. doi: 10.3760/cma.j.issn.1000-6699.2019.08.003. - DOI
-
- 胡 静, 郭 晓玥, 赵 扬玉. 双胎妊娠与母体甲状腺功能的研究进展. 实用妇产科杂志. 2020;36(4):265–267.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical