

Complications of laser-assisted in situ keratomileusis
- PMID: 34146007
- PMCID: PMC8374806
- DOI: 10.4103/ijo.IJO_1872_20
Complications of laser-assisted in situ keratomileusis
Abstract
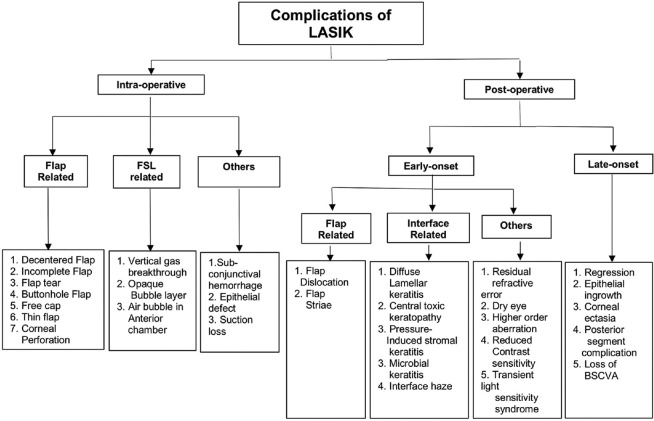
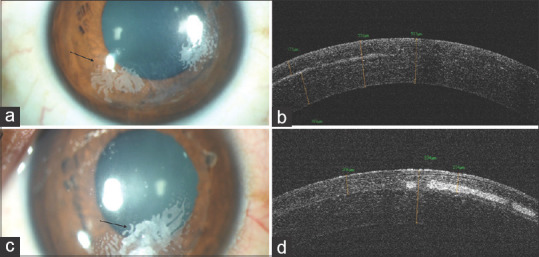
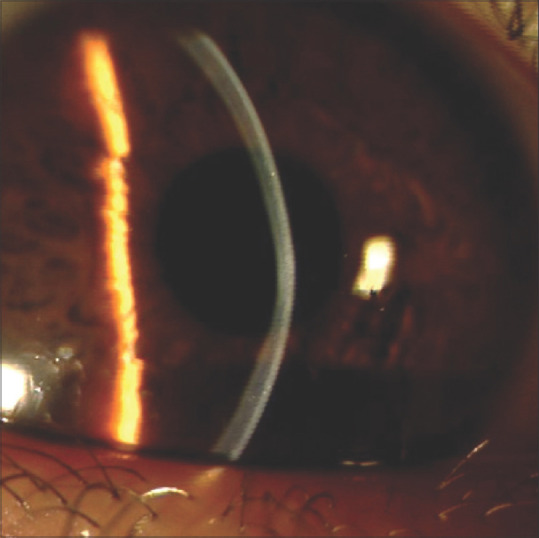
Laser-assisted in situ keratomileusis (LASIK) is one of the most commonly performed kerato-refractive surgery globally. Since its introduction in 1990, there has been a constant evolution in its technology to improve the visual outcome. The safety, efficacy, and predictability of LASIK are well known, but complications with this procedure, although rare, are not unknown. Literature review suggests that intraoperative complications include suction loss, free cap, flap tear, buttonhole flap, decentered ablation, central island, interface debris, femtosecond laser-related complications, and others. The postoperative complications include flap striae, flap dislocation, residual refractive error, diffuse lamellar keratitis, microbial keratitis, epithelial ingrowth, refractive regression, corneal ectasia, and others. This review aims to provide a comprehensive knowledge of risk factors, clinical features, and management protocol of all the reported complications of LASIK. This knowledge will help in prevention as well as early identification and timely intervention with the appropriate strategy for achieving optimal visual outcome even in the face of complications.
Keywords: Diffuse lamellar keratitis; LASIK complications; LASIK; refractive surgery; epithelial ingrowth; flap-related complications; laser in-situ keratomileusis; laser vision correction.
Conflict of interest statement
None
Figures
Comment in
-
Unique complication of femtolasik - A slit buttonhole flap tear.Indian J Ophthalmol. 2022 Jan;70(1):333. doi: 10.4103/ijo.IJO_2093_21. Indian J Ophthalmol. 2022. PMID: 34937276 Free PMC article. No abstract available.
Similar articles
-
Complications of laser-in-situ-keratomileusis.Indian J Ophthalmol. 2002 Dec;50(4):265-82. Indian J Ophthalmol. 2002. PMID: 12532491 Review.
-
[Complications of corneal lamellar refractive surgery].Ophthalmologe. 2015 Dec;112(12):982-9. doi: 10.1007/s00347-015-0172-x. Ophthalmologe. 2015. PMID: 26613941 Review. German.
-
LASIK complications: etiology, management, and prevention.Surv Ophthalmol. 2001 Sep-Oct;46(2):95-116. doi: 10.1016/s0039-6257(01)00254-5. Surv Ophthalmol. 2001. PMID: 11578645 Review.
-
Refractive outcomes of laser in situ keratomileusis after flap complications.J Cataract Refract Surg. 2005 Jul;31(7):1334-7. doi: 10.1016/j.jcrs.2004.11.054. J Cataract Refract Surg. 2005. PMID: 16105603
-
Epithelial ingrowth after late traumatic femtosecond laser-assisted laser in situ keratomileusis flap dislocation.J Cataract Refract Surg. 2019 Dec;45(12):1830-1832. doi: 10.1016/j.jcrs.2019.08.013. J Cataract Refract Surg. 2019. PMID: 31856997
Cited by
-
Diffuse lamellar keratitis as a rare complication of diamond burr superficial keratectomy for recurrent corneal erosion: a case report.BMC Ophthalmol. 2022 Sep 7;22(1):362. doi: 10.1186/s12886-022-02589-3. BMC Ophthalmol. 2022. PMID: 36071403 Free PMC article.
-
Unique complication of femtolasik - A slit buttonhole flap tear.Indian J Ophthalmol. 2022 Jan;70(1):333. doi: 10.4103/ijo.IJO_2093_21. Indian J Ophthalmol. 2022. PMID: 34937276 Free PMC article. No abstract available.
-
Visual and Topographic Outcomes of Corneal Collagen Cross Linking for Post LASIK Ectasia.Clin Ophthalmol. 2022 Jun 20;16:2025-2032. doi: 10.2147/OPTH.S370033. eCollection 2022. Clin Ophthalmol. 2022. PMID: 35757019 Free PMC article.
-
Comparative Analysis of Visual Outcomes and Complications in Intraocular Collamer Lens, Small-Incision Lenticule Extraction, and Laser-Assisted In Situ Keratomileusis Surgeries: A Comprehensive Review.Cureus. 2024 Apr 22;16(4):e58718. doi: 10.7759/cureus.58718. eCollection 2024 Apr. Cureus. 2024. PMID: 38779265 Free PMC article. Review.
-
Evaluating the Rate and Causes of Non-candidacy After Laser-Assisted in Situ Keratomileusis (LASIK) Screening.Cureus. 2025 Jun 23;17(6):e86618. doi: 10.7759/cureus.86618. eCollection 2025 Jun. Cureus. 2025. PMID: 40704251 Free PMC article.
References
-
- Dada T, Sharma N, Vaypayee RB, Dada VK. Subconjuctival hemorrhages after LASIK. Laser in situ keratomileusis. J Cataract Refract Surg. 2000;26:1570 T. - PubMed
-
- Tse SM, Farley ND, Tomasko KR, Amin SR. Intraoperative LASIK Complications. Int Ophthalmol Clin. 2016;56:47e SM. - PubMed
-
- P rez-Santonja JJ, Sakla HF, Ali JL. Contrast sensitivity after laser in situ keratomileusis. J Cataract Refract Surg. 1998;24:183San. - PubMed
-
- Rodrodronja JJ, Sakla HF, Ali JL. Contrast sensitivity after laser in situ keratomileusis. J Cataract Refract Surg 1998;24fract Surg 2he correction of myopia: A contralateral eye study. J Refract Surg. 2010;26:28tral. - PubMed
-
- Moshirfar M, Gardiner JP, Schliesser JA, Espandar L, Feiz V, Mifflin MD, et al. Laser in situ keratomileusis flap complications using mechanical microkeratome versus femtosecond laser:Retrospective comparison. J Cataract Refract Surg. 2010;36:1925riso. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
