

A Randomized Controlled Trial of Heart Failure Disease Management in Skilled Nursing Facilities
- PMID: 34146521
- PMCID: PMC11903054
- DOI: 10.1016/j.jamda.2021.05.023
A Randomized Controlled Trial of Heart Failure Disease Management in Skilled Nursing Facilities
Abstract
Objective: Patients discharged from the hospital to a skilled nursing facility (SNF) are not typically part of a heart failure disease management program (HF-DMP). The objective of this study is to determine if an HF-DMP in SNF improves outcomes for patients with HF.
Design: Cluster-randomized controlled trial.
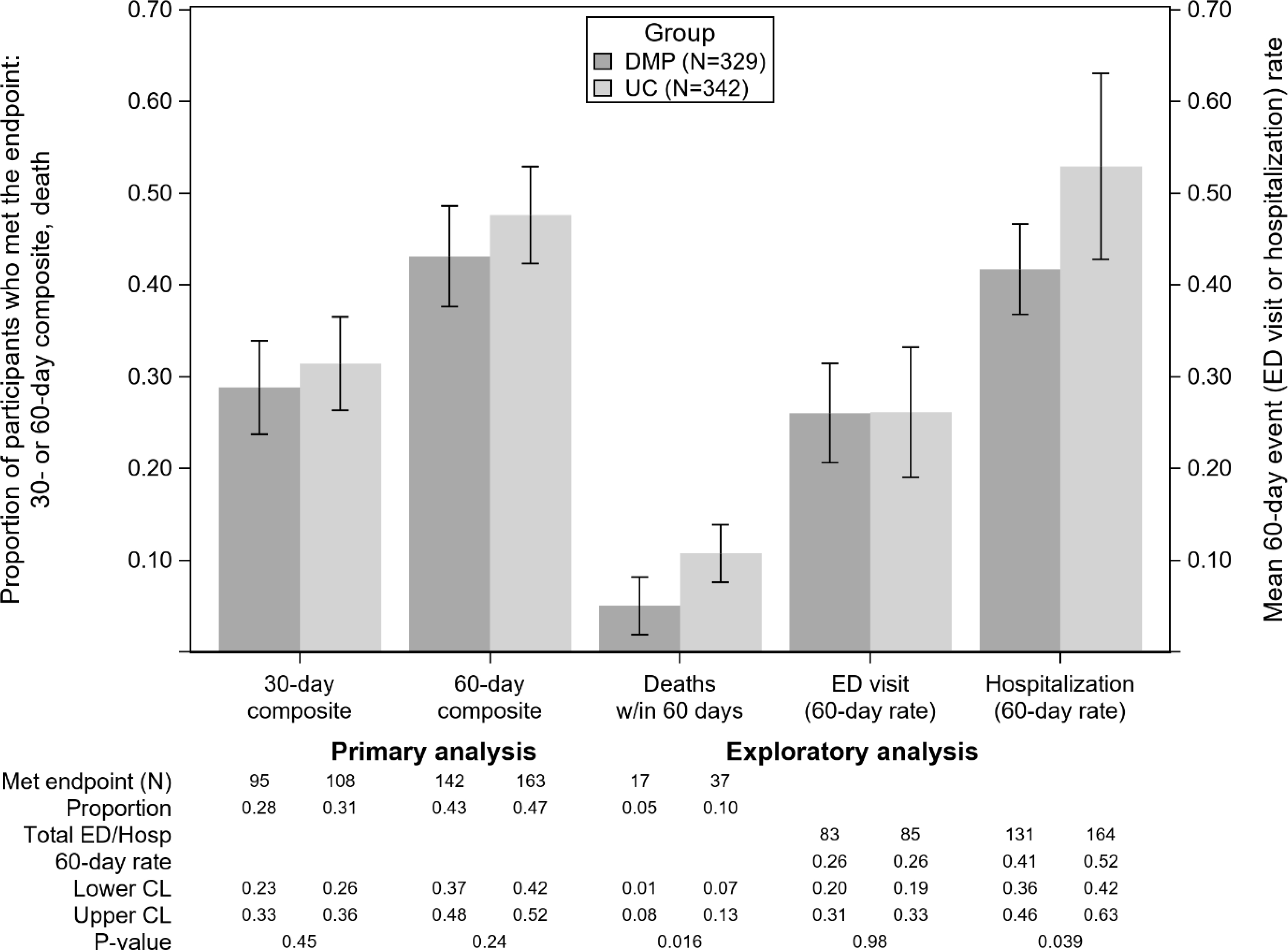
Participants: The trial was conducted in 47 SNFs, and 671 patients were enrolled (329 HF-DMP; 342 to usual care).
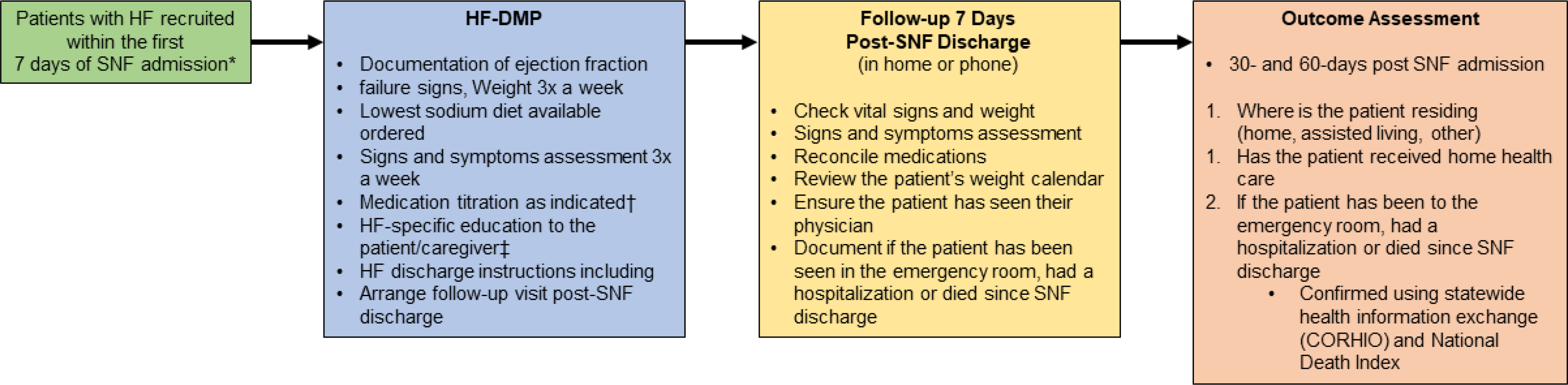
Methods: The HF-DMP included documentation of ejection fraction, symptoms, weights, diet, medication optimization, education, and 7-day visit post SNF discharge. The composite outcome was all-cause hospitalization, emergency department visits, or mortality at 60 days. Secondary outcomes included the composite endpoint at 30 days, change in the Kansas City Cardiomyopathy Questionnaire and the Self-care of HF Index at 60 days. Rehospitalization and mortality rates were calculated as an exploratory outcome.
Results: Mean age of the patients was 79 ± 10 years, 58% were women, and the mean ejection fraction was 51% ± 16%. At 30 and 60 days post SNF admission, the composite endpoint was not significant between DMP (29%) and usual care (32%) at 30 days and 60 days (43% vs 47%, respectively). The Kansas City Cardiomyopathy Questionnaire significantly improved in the HF-DMP vs usual care for the Physical Limitation (11.3 ± 2.9 vs 20.8 ± 3.6; P = .039) and Social Limitation subscales (6.0 ± 3.1 vs 17.9 ± 3.8; P = .016). Self-care of HF Index was not significant. The total number of events (composite endpoint) totaled 517 (231 in HF-DMP and 286 in usual care). Differences in the 60-day hospitalization rate [mean HF-DMP rate 0.43 (SE 0.03) vs usual care 0.54 (SE 0.05), P = .04] and mortality rate (HF-DMP 5.2% vs usual care 10.8%, P < .001) were significant.
Conclusions and implications: The composite endpoint was high for patients with HF in SNF regardless of group. Rehospitalization and mortality rates were reduced by the HF-DMP. HF-DMPs in SNFs may be beneficial to the outcomes of patients with HF. SNFs should consider structured HF-DMPs for their patients.
Keywords: Heart failure disease management; older adults; skilled nursing facilities.
Copyright © 2021 AMDA – The Society for Post-Acute and Long-Term Care Medicine. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
All authors had no conflicts of interest.
Figures
References
-
- Hines ALBM, Jiang J, Steiner CA. Conditions with the largest number of adult hospital readmissions by payer, 2011. Agency for Healthcare Research and Quality;2014. - PubMed
-
- Services CfMaM. The skilled nursing facility value-based purchasing program (SNF VBP). 2018; https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Inst.... Accessed December 6, 2018.
-
- Commission MPA. Skilled nursing facility services. 2017; http://www.medpac.gov/docs/defaultsource/reports/mar17_medpac_ch8.pdf. Accessed December 6, 2018.
-
- Rich MW, Beckham V, Wittenberg C, Leven CL, Freedland KE, Carney RM. A multidisciplinary intervention to prevent the readmission of elderly patients with congestive heart failure. N Engl J Med 1995;333(18):1190–1195. - PubMed
-
- Stewart S, Horowitz JD. Home-based intervention in congestive heart failure: long-term implications on readmission and survival. Circulation. 2002;105(24):2861–2866. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
