

Impact of COVID-19 on Cardiovascular Testing in the United States Versus the Rest of the World
- PMID: 34147434
- PMCID: PMC8374310
- DOI: 10.1016/j.jcmg.2021.03.007
Impact of COVID-19 on Cardiovascular Testing in the United States Versus the Rest of the World
Abstract
Objectives: This study sought to quantify and compare the decline in volumes of cardiovascular procedures between the United States and non-U.S. institutions during the early phase of the coronavirus disease-2019 (COVID-19) pandemic.
Background: The COVID-19 pandemic has disrupted the care of many non-COVID-19 illnesses. Reductions in diagnostic cardiovascular testing around the world have led to concerns over the implications of reduced testing for cardiovascular disease (CVD) morbidity and mortality.
Methods: Data were submitted to the INCAPS-COVID (International Atomic Energy Agency Non-Invasive Cardiology Protocols Study of COVID-19), a multinational registry comprising 909 institutions in 108 countries (including 155 facilities in 40 U.S. states), assessing the impact of the COVID-19 pandemic on volumes of diagnostic cardiovascular procedures. Data were obtained for April 2020 and compared with volumes of baseline procedures from March 2019. We compared laboratory characteristics, practices, and procedure volumes between U.S. and non-U.S. facilities and between U.S. geographic regions and identified factors associated with volume reduction in the United States.
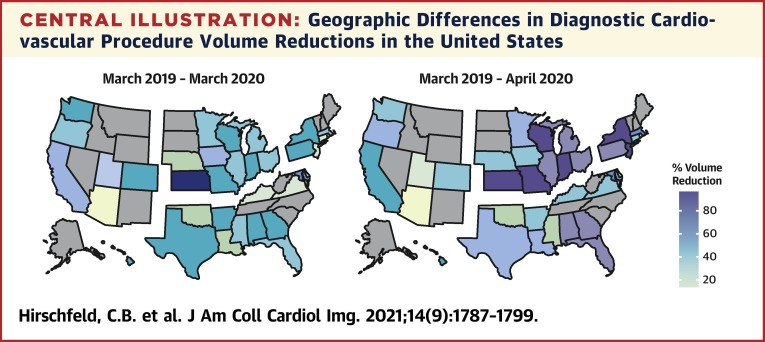
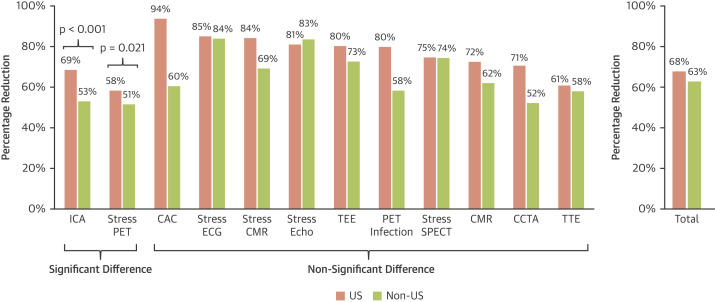
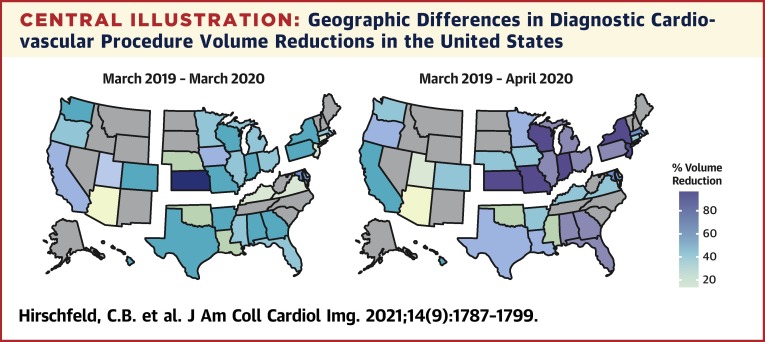
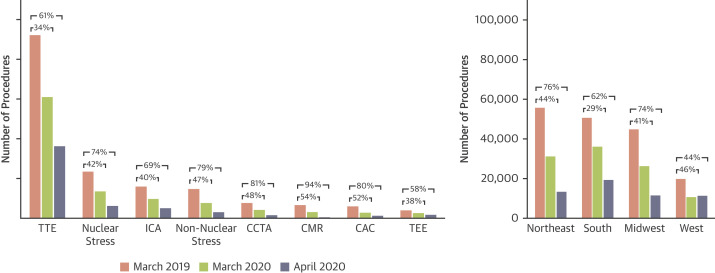
Results: Reductions in the volumes of procedures in the United States were similar to those in non-U.S. facilities (68% vs. 63%, respectively; p = 0.237), although U.S. facilities reported greater reductions in invasive coronary angiography (69% vs. 53%, respectively; p < 0.001). Significantly more U.S. facilities reported increased use of telehealth and patient screening measures than non-U.S. facilities, such as temperature checks, symptom screenings, and COVID-19 testing. Reductions in volumes of procedures differed between U.S. regions, with larger declines observed in the Northeast (76%) and Midwest (74%) than in the South (62%) and West (44%). Prevalence of COVID-19, staff redeployments, outpatient centers, and urban centers were associated with greater reductions in volume in U.S. facilities in a multivariable analysis.
Conclusions: We observed marked reductions in U.S. cardiovascular testing in the early phase of the pandemic and significant variability between U.S. regions. The association between reductions of volumes and COVID-19 prevalence in the United States highlighted the need for proactive efforts to maintain access to cardiovascular testing in areas most affected by outbreaks of COVID-19 infection.
Keywords: COVID-19; cardiovascular disease; cardiovascular imaging; coronavirus; diagnostic cardiovascular procedure.
Copyright © 2021 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures This work was supported by the International Atomic Energy Agency. Dr. Blankstein has previously received research support from Amgen and Astellas Inc. Dr. Ferencik has been previously supported by U.S. National Institutes of Health (NIH) and American Heart Association; and is a consultant for Biograph, Inc. Dr. Nørgaard has previously received unrestricted institutional research grants from Siemens and HeartFlow. Dr. Maurovich-Horvat has been a shareholder of Neumann Medical Ltd. Dr. Einstein has previously received grants from NIH, International Atomic Energy Agency, Canon Medical Systems, Roche Medical Systems, WL Gore, and GE Health care; consultant for WL Gore; on the Speakers Bureau for Ionetix; has received travel/accommodations/meeting expenses from HeartFlow; and is a stockholder in Emergent BioSolutions Inc. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Comment in
-
The Cardiovascular Imaging Community's Response to the COVID-19 Pandemic.JACC Cardiovasc Imaging. 2021 Sep;14(9):1800-1803. doi: 10.1016/j.jcmg.2021.04.002. Epub 2021 Jun 16. JACC Cardiovasc Imaging. 2021. PMID: 34147460 Free PMC article.
References
-
- Keesara S., Jonas A., Schulman K. Covid-19 and health care's digital revolution. N Engl J Med. 2020;382:e82. - PubMed
-
- Anteby R., Zager Y., Barash Y., et al. The impact of the coronavirus disease 2019 outbreak on the attendance of patients with surgical complaints at a tertiary hospital emergency department. J Laparoendosc Adv Surg Tech A. 2020;30(9):1001–1007. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
