

Early Tracheostomy for Managing ICU Capacity During the COVID-19 Outbreak: A Propensity-Matched Cohort Study
- PMID: 34147502
- PMCID: PMC8361308
- DOI: 10.1016/j.chest.2021.06.015
Early Tracheostomy for Managing ICU Capacity During the COVID-19 Outbreak: A Propensity-Matched Cohort Study
Abstract
Background: During the first wave of the COVID-19 pandemic, shortages of ventilators and ICU beds overwhelmed health care systems. Whether early tracheostomy reduces the duration of mechanical ventilation and ICU stay is controversial.
Research question: Can failure-free day outcomes focused on ICU resources help to decide the optimal timing of tracheostomy in overburdened health care systems during viral epidemics?
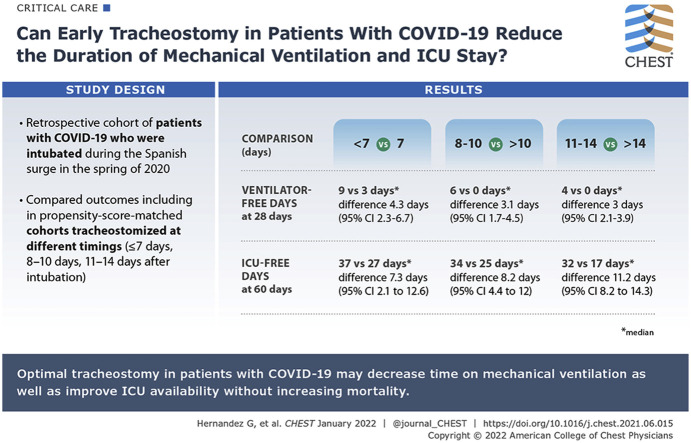
Study design and methods: This retrospective cohort study included consecutive patients with COVID-19 pneumonia who had undergone tracheostomy in 15 Spanish ICUs during the surge, when ICU occupancy modified clinician criteria to perform tracheostomy in Patients with COVID-19. We compared ventilator-free days at 28 and 60 days and ICU- and hospital bed-free days at 28 and 60 days in propensity score-matched cohorts who underwent tracheostomy at different timings (≤ 7 days, 8-10 days, and 11-14 days after intubation).
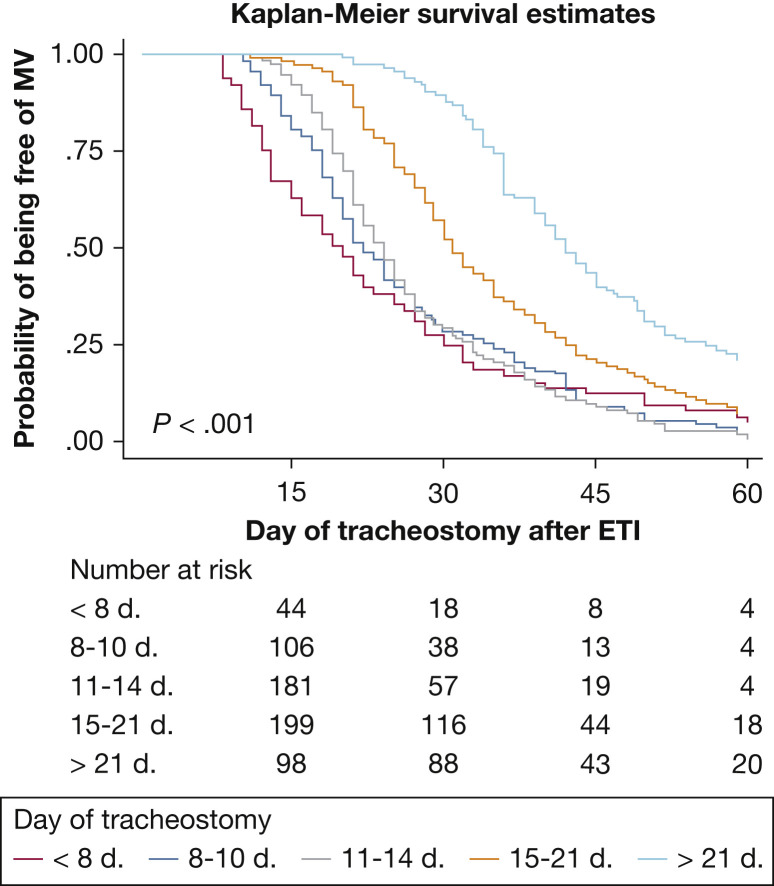
Results: Of 1,939 patients admitted with COVID-19 pneumonia, 682 (35.2%) underwent tracheostomy, 382 (56%) within 14 days. Earlier tracheostomy was associated with more ventilator-free days at 28 days (≤ 7 days vs > 7 days [116 patients included in the analysis]: median, 9 days [interquartile range (IQR), 0-15 days] vs 3 days [IQR, 0-7 days]; difference between groups, 4.5 days; 95% CI, 2.3-6.7 days; 8-10 days vs > 10 days [222 patients analyzed]: 6 days [IQR, 0-10 days] vs 0 days [IQR, 0-6 days]; difference, 3.1 days; 95% CI, 1.7-4.5 days; 11-14 days vs > 14 days [318 patients analyzed]: 4 days [IQR, 0-9 days] vs 0 days [IQR, 0-2 days]; difference, 3 days; 95% CI, 2.1-3.9 days). Except hospital bed-free days at 28 days, all other end points were better with early tracheostomy.
Interpretation: Optimal timing of tracheostomy may improve patient outcomes and may alleviate ICU capacity strain during the COVID-19 pandemic without increasing mortality. Tracheostomy within the first work on a ventilator in particular may improve ICU availability.
Keywords: capacity; failure-free; resource; timing; tracheostomy.
Copyright © 2021 American College of Chest Physicians. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
From Fog of War to Tailored Tracheostomy Timing.Chest. 2022 Jan;161(1):8-10. doi: 10.1016/j.chest.2021.07.2173. Chest. 2022. PMID: 35000709 No abstract available.
-
Early Tracheostomy as a Strategy for Capacity Strain Must Be More Thoughtfully Considered.Chest. 2022 Jun;161(6):e395-e396. doi: 10.1016/j.chest.2022.01.067. Chest. 2022. PMID: 35680327 No abstract available.
-
Response.Chest. 2022 Jun;161(6):e396. doi: 10.1016/j.chest.2022.01.068. Chest. 2022. PMID: 35680328 No abstract available.
References
-
- McGrath B.A., Wallace S., Goswamy J. Laryngeal oedema associated with COVID-19 complicating airway management. Anaesthesia. 2020;75:962–977. - PubMed
-
- Wang R., Pan C., Wang X., Xu F., Jiang S., Li M. The impact of tracheostomy in critically ill patients undergoing mechanical ventilation: a meta-analysis of randomized controlled clinical trials with trial sequential analysis. Heart Lung. 2019;48:46–54. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
