

A Molecular Signature Response Classifier to Predict Inadequate Response to Tumor Necrosis Factor-α Inhibitors: The NETWORK-004 Prospective Observational Study
- PMID: 34148193
- PMCID: PMC8214458
- DOI: 10.1007/s40744-021-00330-y
A Molecular Signature Response Classifier to Predict Inadequate Response to Tumor Necrosis Factor-α Inhibitors: The NETWORK-004 Prospective Observational Study
Abstract
Introduction: Timely matching of patients to beneficial targeted therapy is an unmet need in rheumatoid arthritis (RA). A molecular signature response classifier (MSRC) that predicts which patients with RA are unlikely to respond to tumor necrosis factor-α inhibitor (TNFi) therapy would have wide clinical utility.
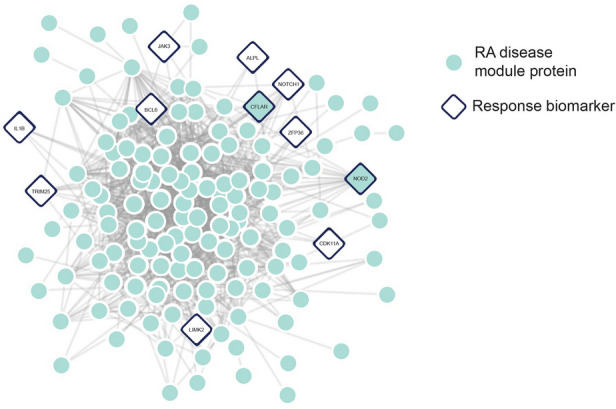
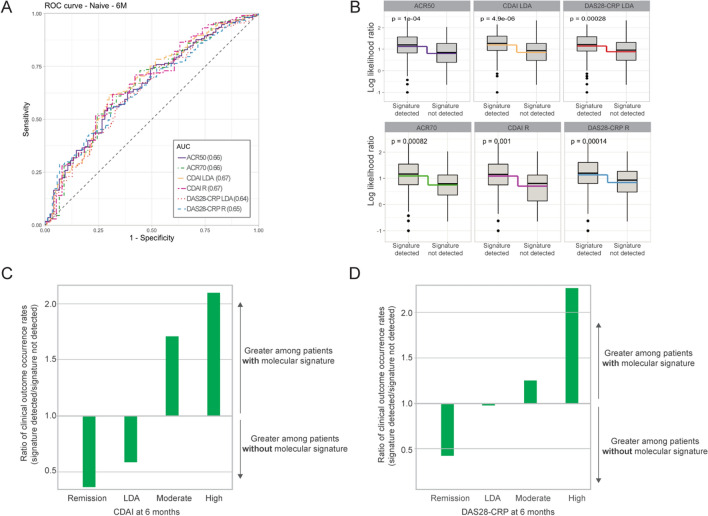
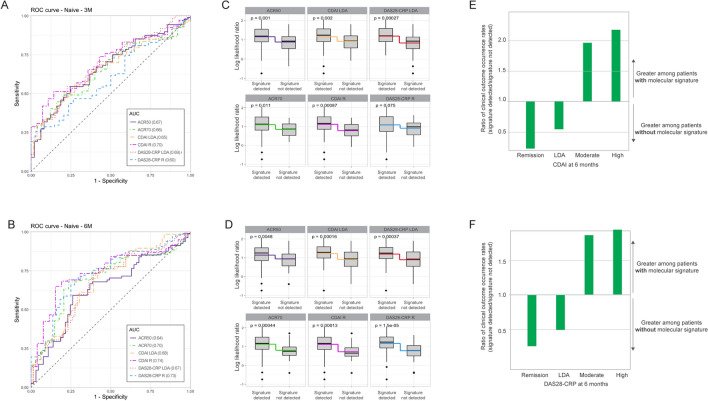
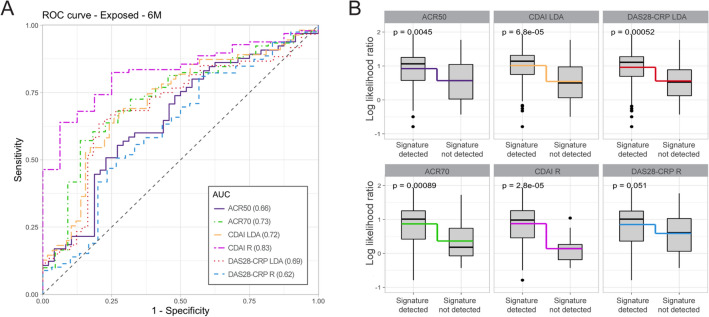
Methods: The protein-protein interaction map specific to the rheumatoid arthritis pathophysiology and gene expression data in blood patient samples was used to discover a molecular signature of non-response to TNFi therapy. Inadequate response predictions were validated in blood samples from the CERTAIN cohort and a multicenter blinded prospective observational clinical study (NETWORK-004) among 391 targeted therapy-naïve and 113 TNFi-exposed patient samples. The primary endpoint evaluated the ability of the MSRC to identify patients who inadequately responded to TNFi therapy at 6 months according to ACR50. Additional endpoints evaluated the prediction of inadequate response at 3 and 6 months by ACR70, DAS28-CRP, and CDAI.
Results: The 23-feature molecular signature considers pathways upstream and downstream of TNFα involvement in RA pathophysiology. Predictive performance was consistent between the CERTAIN cohort and NETWORK-004 study. The NETWORK-004 study met primary and secondary endpoints. A molecular signature of non-response was detected in 45% of targeted therapy-naïve patients. The MSRC had an area under the curve (AUC) of 0.64 and patients were unlikely to adequately respond to TNFi therapy according to ACR50 at 6 months with an odds ratio of 4.1 (95% confidence interval 2.0-8.3, p value 0.0001). Odds ratios (3.4-8.8) were significant (p value < 0.01) for additional endpoints at 3 and 6 months, with AUC values up to 0.74. Among TNFi-exposed patients, the MSRC had an AUC of up to 0.83 and was associated with significant odds ratios of 3.3-26.6 by ACR, DAS28-CRP, and CDAI metrics.
Conclusion: The MSRC stratifies patients according to likelihood of inadequate response to TNFi therapy and provides patient-specific data to guide therapy choice in RA for targeted therapy-naïve and TNFi-exposed patients.
Keywords: Drug response prediction; Gene expression; Precision medicine; Prospective observational study; Rheumatoid arthritis; TNF inhibitor.
Plain language summary
A blood-based molecular signature response classifier (MSRC) integrating next-generation RNA sequencing data with clinical features predicts the likelihood that a patient with rheumatoid arthritis will have an inadequate response to TNFi therapy. Treatment selection guided by test results, with likely inadequate responders appropriately redirected to a different therapy, could improve response rates to TNFi therapies, generate healthcare cost savings, and increase rheumatologists’ confidence in prescribing decisions and altered treatment choices. The MSRC described in this study predicts the likelihood of inadequate response to TNFi therapies among targeted therapy-naïve and TNFi-exposed patients in a multicenter, 24-week blinded prospective clinical study: NETWORK-004. Patients with a molecular signature of non-response are less likely to have an adequate response to TNFi therapies than those patients lacking the signature according to ACR50, ACR70, CDAI, and DAS28-CRP with significant odds ratios of 3.4–8.8 for targeted therapy-naïve patients and 3.3–26.6 for TNFi-exposed patients. This MSRC provides a solution to the long-standing need for precision medicine tools to predict drug response in rheumatoid arthritis—a heterogeneous and progressive disease with an abundance of therapeutic options. These data validate the performance of the MSRC in a blinded prospective clinical study of targeted therapy-naïve and TNFi therapy-exposed patients.
© 2021. The Author(s).
Figures
References
-
- Smolen JS, Landewe RBM, Bijlsma JWJ, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2019 update. Ann Rheum Dis. 2020;79(6):685–99. - PubMed
-
- Aletaha D. Precision medicine and management of rheumatoid arthritis. J Autoimmun. 2020;110:102405. - PubMed
-
- Bluett J, Barton A. Precision medicine in rheumatoid arthritis. Rheum Dis Clin North Am. 2017;43(3):377–387. - PubMed
-
- Singh JA, Saag KG, Bridges SL, Jr, et al. 2015 American College of Rheumatology guideline for the treatment of rheumatoid arthritis. Arthritis Rheumatol. 2016;68(1):1–26. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
