

doi: 10.1161/HYPERTENSIONAHA.120.16181.
Epub 2021 Jun 21.
Association of Apparent Treatment-Resistant Hypertension With Differential Risk of End-Stage Kidney Disease Across Racial Groups in the Million Veteran Program
Affiliations
- PMID: 34148359
- PMCID: PMC8364328
- DOI: 10.1161/HYPERTENSIONAHA.120.16181
Item in Clipboard
Association of Apparent Treatment-Resistant Hypertension With Differential Risk of End-Stage Kidney Disease Across Racial Groups in the Million Veteran Program
Hypertension.
2021 Aug.
Abstract
[Figure: see text].
Keywords: Treatment-resistant hypertension; apolipoprotein L1 variants; end-stage kidney disease; myocardial infarction; race; stroke.
Figures
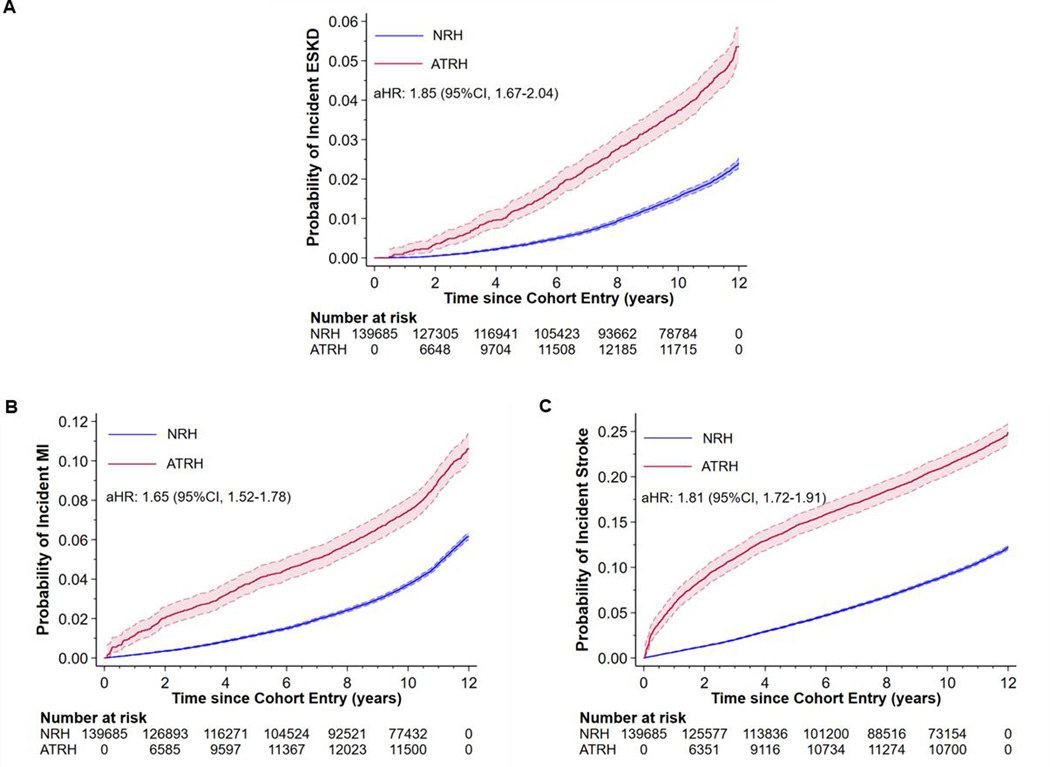
Effect of apparent treatment resistant hypertension (ATRH) on the risk of incident ESKD, MI and stroke among hypertensive Veterans in the Million Veteran Program. After full adjustment for baseline covariates, compared to NRH, ATRH was associated with an 85%, 65% and 81% higher risk of incident ESKD, MI and stroke respectively. Abbreviations: ATRH, apparent treatment resistant hypertension; ESKD, end-stage kidney disease; MI, myocardial infarction; NRH, non-resistant hypertension.
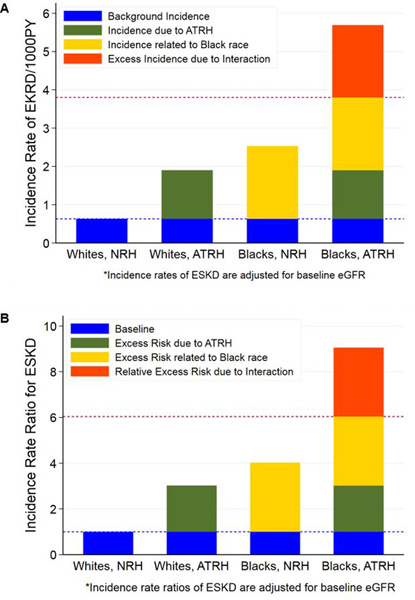
A. Excess incidence of incident ESKD due to interaction between ATRH and race. In the absence of interaction, the expected incidence rate (per 1000PY) among blacks with ATRH would be the sum of the background incidence (0.63), incidence due to ATRH alone (1.27) and incidence related to black race (1.90). However, the observed incidence (5.69) was greater than the expected (3.80); which is suggestive of synergistic additive interaction between ATRH and black race for the association with incident ESKD. The excess incidence due to interaction (dark orange bar) represents an excess of 189 incident ESKD cases per 100, 000PY among blacks with ATRH. Abbreviations: ATRH, apparent treatment resistant hypertension; ESKD, end-stage kidney disease; NRH, non-resistant hypertension; PY, person-years. B. Relative excess risk of incident ESKD due to interaction between ATRH and race. The Y-axis represents the incidence rate ratio (IRR) for ESKD comparing whites with ATRH, blacks with NRH, blacks with ATRH to the referent group (whites with NRH). The relative excess risk due to interaction (RERI) between ATRH and race = IRR11 - IRR10 - IRR01 + 1 = 3.00 (95%CI: 1.79, 4.21); and is represented by the dark orange bar as in Figure 2A. The attributable proportion (AP) = RERI/IRR11 = 33.2 (95%CI: 23.6, 42.7) suggesting that 33.2% of the risk of incident ESKD among blacks with ATRH is due to the synergistic interaction between ATRH and race. Abbreviations: ATRH, apparent treatment resistant hypertension; ESKD, end-stage kidney disease; NRH, non-resistant hypertension.
References
-
- United States Renal Data System. 2018 USRDS annual data report: Epidemiology of kidney disease in the United States. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD, 2018.
-
- Benjamin EJ, Virani SS, Callaway CW, Chamberlain AM, Chang AR, Cheng S, Chiuve SE, Cushman M, Delling FN, Deo R, de Ferranti SD, Ferguson JF, Fornage M, Gillespie C, Isasi CR, Jimenez MC, Jordan LC, Judd SE, Lackland D, Lichtman JH, Lisabeth L, Liu S, Longenecker CT, Lutsey PL, Mackey JS, Matchar DB, Matsushita K, Mussolino ME, Nasir K, O’Flaherty M, Palaniappan LP, Pandey A, Pandey DK, Reeves MJ, Ritchey MD, Rodriguez CJ, Roth GA, Rosamond WD, Sampson UKA, Satou GM, Shah SH, Spartano NL, Tirschwell DL, Tsao CW, Voeks JH, Willey JZ, Wilkins JT, Wu JH, Alger HM, Wong SS and Muntner P. Heart Disease and Stroke Statistics-2018 Update: A Report From the American Heart Association. Circulation. 2018;137:e67–e492. - PubMed
-
- Carey RM, Calhoun DA, Bakris GL, Brook RD, Daugherty SL, Dennison-Himmelfarb CR, Egan BM, Flack JM, Gidding SS, Judd E, Lackland DT, Laffer CL, Newton-Cheh C, Smith SM, Taler SJ, Textor SC, Turan TN and White WB. Resistant Hypertension: Detection, Evaluation, and Management: A Scientific Statement From the American Heart Association. Hypertension. 2018;72:e53–e90. - PMC - PubMed
-
- Tanner RM, Calhoun DA, Bell EK, Bowling CB, Gutierrez OM, Irvin MR, Lackland DT, Oparil S, McClellan W, Warnock DG and Muntner P. Incident ESRD and treatment-resistant hypertension: the reasons for geographic and racial differences in stroke (REGARDS) study. Am J Kidney Dis. 2014;63:781–8. - PMC - PubMed
-
- Muntner P, Davis BR, Cushman WC, Bangalore S, Calhoun DA, Pressel SL, Black HR, Kostis JB, Probstfield JL, Whelton PK, Rahman M and Group ACR. Treatment-resistant hypertension and the incidence of cardiovascular disease and end-stage renal disease: results from the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT). Hypertension. 2014;64:1012–21. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
