

Longitudinal changes in extent of late gadolinium enhancement in repaired Tetralogy of Fallot: a retrospective analysis of serial CMRs
- PMID: 34148557
- PMCID: PMC8215816
- DOI: 10.1186/s12968-021-00772-x
Longitudinal changes in extent of late gadolinium enhancement in repaired Tetralogy of Fallot: a retrospective analysis of serial CMRs
Abstract
Background: Right ventricular (RV) late gadolinium enhancement (LGE) occurs due to surgical scarring and RV remodeling, and has been shown to be associated with clinical outcomes in Tetralogy of Fallot (TOF). However, it is not known if cardiovascular magnetic resonance (CMR) LGE extent progresses over time, and therefore, it is not known if serial reassessment of LGE is necessary. We determined the rate of progression in the extent of RV LGE on serial CMR examinations in repaired TOF.
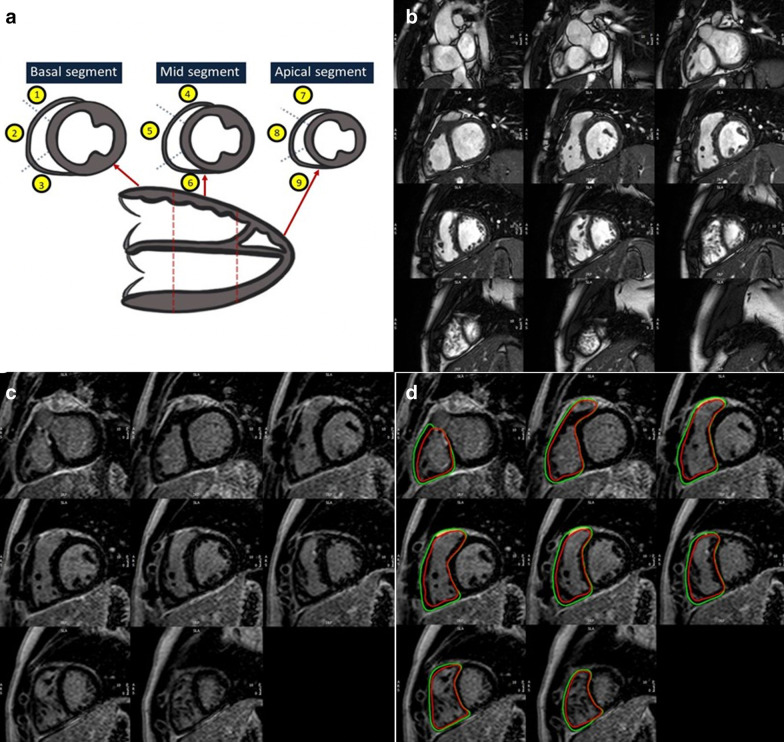
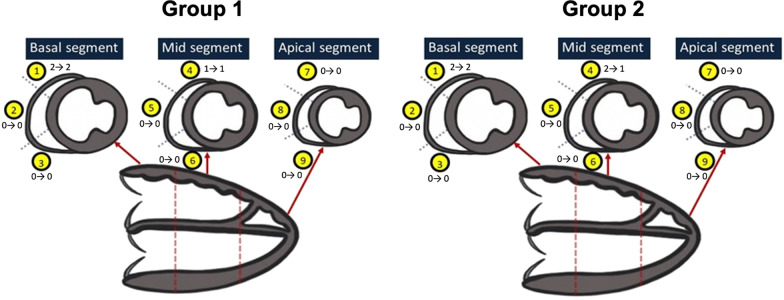
Methods: Retrospective review of 127 patients after TOF repair (49% male, median age at first CMR 18.9 years (Interquartile range (IQR) 13.3,27.0) who had at least two CMRs (median follow-up duration of 4.0 years (IQR 2.1,5.9)) was performed. 84/127 patients had no interventions between serial CMRs (Group 1) while 43/127 patients had transcatheter or surgical intervention between CMRs (Group 2). The extent of RV LGE was assessed using 2 methods: a semiquantitative RV LGE score and a quantitative RV LGE extent expressed as % of RV mass. Mixed effects linear regression modeling to estimate changes in LGE over time.
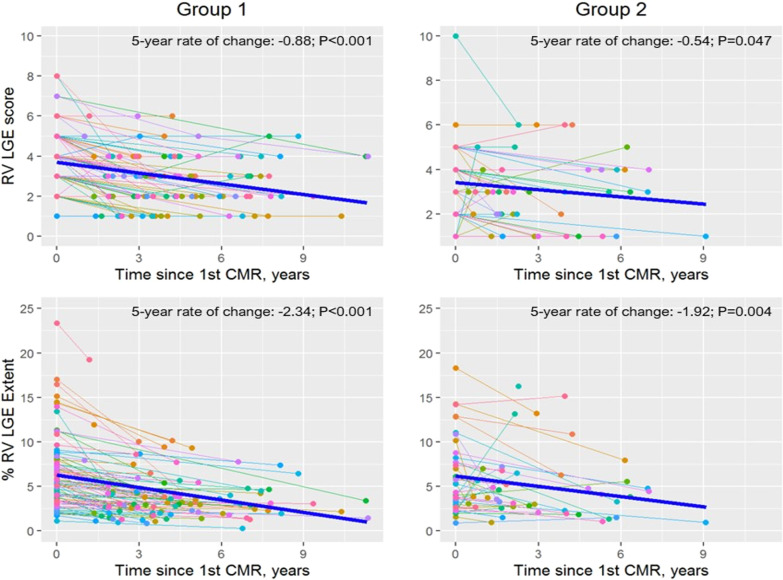
Results: RV LGE was present in all patients on the first CMR. % RV LGE extent and LGE score did not increase over time in either patient group. The mean 5 year rates of change were small and negative for both % RV LGE extent [- 2.3 (95% CI - 2.9, - 1.8, p < 0.001) in Group 1, and - 1.9 (95% CI - 3.2, - 0.7, p = 0.004) in Group 2], and RV LGE score [- 0.9 (95% CI - 1.1, - 0.6, p < 0.001) in Group 1, and - 0.5 (95% CI - 1.1, - 0.0, p = 0.047) in Group 2].
Conclusions: In this serial CMR evaluation of children and adults with repaired TOF, no significant progression in the extent of RV LGE was seen on intermediate term follow-up. Given recent concerns regarding the safety of gadolinium-based contrast agents, frequent assessment of LGE may not be necessary in follow-up.
Keywords: Cardiovascular magnetic resonance; Late gadolinium enhancement; Longitudinal study; Tetralogy of Fallot.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
The predictive role of right ventricular late gadolinium enhancement in patients with tetralogy of Fallot undergoing pulmonary valve replacement.Eur Radiol Exp. 2023 Feb 24;7(1):9. doi: 10.1186/s41747-023-00322-3. Eur Radiol Exp. 2023. PMID: 36826698 Free PMC article.
-
Relation of fragmented QRS complex to right ventricular fibrosis detected by late gadolinium enhancement cardiac magnetic resonance in adults with repaired tetralogy of fallot.Am J Cardiol. 2012 Jan 1;109(1):110-5. doi: 10.1016/j.amjcard.2011.07.070. Epub 2011 Sep 29. Am J Cardiol. 2012. PMID: 21962997
-
Three-Dimensional Late Gadolinium Enhancement Cardiovascular Magnetic Resonance Predicts Inducibility of Ventricular Tachycardia in Adults With Repaired Tetralogy of Fallot.Circ Arrhythm Electrophysiol. 2020 Nov;13(11):e008321. doi: 10.1161/CIRCEP.119.008321. Epub 2020 Oct 6. Circ Arrhythm Electrophysiol. 2020. PMID: 33022183
-
Late gadolinium enhancement in patients with Tetralogy of Fallot: A systematic review.Eur J Radiol. 2021 Mar;136:109521. doi: 10.1016/j.ejrad.2021.109521. Epub 2021 Jan 6. Eur J Radiol. 2021. PMID: 33450661
-
Prediction of ventricular arrhythmias using cardiovascular magnetic resonance.Eur Heart J Cardiovasc Imaging. 2013 Jun;14(6):518-25. doi: 10.1093/ehjci/jes302. Epub 2013 Jan 16. Eur Heart J Cardiovasc Imaging. 2013. PMID: 23324829 Review.
Cited by
-
Myocardial Fibrosis in Congenital Heart Disease and the Role of MRI.Radiol Cardiothorac Imaging. 2023 Jun 1;5(3):e220255. doi: 10.1148/ryct.220255. eCollection 2023 Jun. Radiol Cardiothorac Imaging. 2023. PMID: 37404787 Free PMC article. Review.
-
Repaired Tetralogy of Fallot: Have We Understood the Right Timing of PVR?J Clin Med. 2024 May 2;13(9):2682. doi: 10.3390/jcm13092682. J Clin Med. 2024. PMID: 38731211 Free PMC article. Review.
-
The predictive role of right ventricular late gadolinium enhancement in patients with tetralogy of Fallot undergoing pulmonary valve replacement.Eur Radiol Exp. 2023 Feb 24;7(1):9. doi: 10.1186/s41747-023-00322-3. Eur Radiol Exp. 2023. PMID: 36826698 Free PMC article.
-
Contemporary multimodality non-invasive cardiac imaging protocols for tetralogy of Fallot.Pediatr Radiol. 2024 Jun;54(7):1075-1092. doi: 10.1007/s00247-024-05942-4. Epub 2024 May 23. Pediatr Radiol. 2024. PMID: 38782776 Review.
References
-
- Stirrat J, Rajchl M, Bergin L, Patton DJ, Peters T, White JA. High-resolution 3-dimensional late gadolinium enhancement scar imaging in surgically corrected Tetralogy of Fallot: clinical feasibility of volumetric quantification and visualization. J Cardiovasc Magn Reson. 2014;16:76. doi: 10.1186/s12968-014-0076-y. - DOI - PMC - PubMed
-
- Khairy P, Landzberg MJ, Gatzoulis MA, Lucron H, Lambert J, Marcon F, Alexander ME, Walsh EP. Value of programmed ventricular stimulation after Tetralogy of Fallot repair: a multicenter study. Circulation. 2004;109:1994–2000. doi: 10.1161/01.CIR.0000126495.11040.BD. - DOI - PubMed
-
- Geva T, Mulder B, Gauvreau K, Babu-Narayan SV, Wald RM, Hickey K, Powell AJ, Gatzoulis MA, Valente AM. Preoperative predictors of death and sustained ventricular tachycardia after pulmonary valve replacement in patients with repaired Tetralogy of Fallot enrolled in the INDICATOR Cohort. Circulation. 2018;138:2106–2115. doi: 10.1161/CIRCULATIONAHA.118.034740. - DOI - PubMed
-
- Valente AM, Gauvreau K, Assenza GE, Babu-Narayan SV, Schreier J, Gatzoulis MA, Groenink M, Inuzuka R, Kilner PJ, Koyak Z, Landzberg MJ, Mulder B, Powell AJ, Wald R, Geva T. Contemporary predictors of death and sustained ventricular tachycardia in patients with repaired Tetralogy of Fallot enrolled in the INDICATOR cohort. Heart. 2014;100:247–253. doi: 10.1136/heartjnl-2013-304958. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
