

Long Spinal Cord Lesions Caused by Venous Congestive Myelopathy Associated with Intravascular Large B-cell Lymphoma
- PMID: 34148949
- PMCID: PMC8710383
- DOI: 10.2169/internalmedicine.6717-20
Long Spinal Cord Lesions Caused by Venous Congestive Myelopathy Associated with Intravascular Large B-cell Lymphoma
Abstract
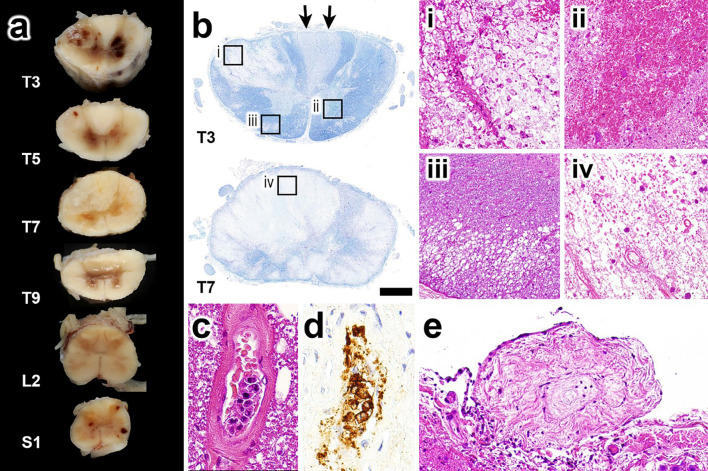
Intravascular large B-cell lymphoma (IVLBCL) is a subtype of B-cell lymphoma, characterized by lymphoma cell proliferation within small blood vessels. We herein describe a rare case with long spinal cord lesions caused by venous congestive myelopathy associated with IVLBCL. An 81-year-old man presented with paraplegia of the lower limbs and sensory disturbances. Magnetic resonance imaging revealed intramedullary longitudinal T2-hyperintensity lesions in the thoracic cords. The patient died three months after disease onset, and a neuropathological analysis revealed predominantly atypical B-lymphocytes located sparsely in the veins of the spinal cord. IVLBCL should be considered in the differential diagnoses of long spinal cord lesions.
Keywords: IVL; IVLBCL; MALT lymphoma; intravascular lymphoma; long spinal cord lesion; venous congestive myelopathy.
Conflict of interest statement
Figures



Similar articles
-
[Case of intravascular lymphoma with a longitudinal spinal lesion diagnosed by multiple biopsies].Rinsho Shinkeigaku. 2012;52(5):336-43. doi: 10.5692/clinicalneurol.52.336. Rinsho Shinkeigaku. 2012. PMID: 22688113 Review. Japanese.
-
[A case of primary intramedullary spinal cord lymphoma diagnosed by spinal cord biopsy of long spinal cord lesions showing persistent gadolinium contrast enhancement].Rinsho Shinkeigaku. 2021 Dec 22;61(12):856-861. doi: 10.5692/clinicalneurol.cn-001655. Epub 2021 Nov 18. Rinsho Shinkeigaku. 2021. PMID: 34789630 Japanese.
-
Progressive conus medullaris lesions are suggestive of intravascular large B-cell lymphoma.Eur J Neurol. 2023 Oct;30(10):3236-3243. doi: 10.1111/ene.15941. Epub 2023 Jul 4. Eur J Neurol. 2023. PMID: 37350144
-
[Intravascular large B-cell lymphoma with low signal intensity lesions on T2 weighted spinal magnetic resonance image that were suspected to be hemorrhages].Rinsho Shinkeigaku. 2012;52(5):344-50. doi: 10.5692/clinicalneurol.52.344. Rinsho Shinkeigaku. 2012. PMID: 22688114 Japanese.
-
Intravascular lymphoma forming massive aortic tumors complicated with sarcoidosis and focal segmental glomerulosclerosis: a case report and literature review.BMC Nephrol. 2018 Oct 29;19(1):300. doi: 10.1186/s12882-018-1106-z. BMC Nephrol. 2018. PMID: 30373554 Free PMC article. Review.
Cited by
-
Intravascular Large B-Cell Lymphoma: A Review with a Focus on the Prognostic Value of Skin Involvement.Curr Oncol. 2022 Apr 19;29(5):2909-2919. doi: 10.3390/curroncol29050237. Curr Oncol. 2022. PMID: 35621627 Free PMC article. Review.
-
Magnetic resonance imaging findings of intravascular large B-cell lymphoma mimicking fasciitis of the thigh: A case report.J Clin Exp Hematop. 2025 Jun 28;65(2):115-120. doi: 10.3960/jslrt.24072. Epub 2025 Apr 30. J Clin Exp Hematop. 2025. PMID: 40301079 Free PMC article.
References
-
- Sukswai N, Lyapichev K, Khoury JD, Medeiros LJ. Diffuse large B-cell lymphoma variants: an update. Pathology 52: 53-67, 2020. - PubMed
-
- Takizawa S, Shirasugi Y, Nakamura N, et al. . An atypical form of Asian variant of intravascular large B-cell lymphoma presenting with myelopathy alone for 4 months prior to pancytopenia. Intern Med 46: 1879-1880, 2007. - PubMed
-
- Kumar N, Keegan BM, Rodriguez FJ, Hammack JE, Kantarci OH. Intravascular lymphoma presenting as a longitudinally-extensive myelitis: diagnostic challenges and etiologic clues. J Neurol Sci 303: 146-149, 2011. - PubMed