

Inefficient Placental Virus Replication and Absence of Neonatal Cell-Specific Immunity Upon Sars-CoV-2 Infection During Pregnancy
- PMID: 34149740
- PMCID: PMC8211452
- DOI: 10.3389/fimmu.2021.698578
Inefficient Placental Virus Replication and Absence of Neonatal Cell-Specific Immunity Upon Sars-CoV-2 Infection During Pregnancy
Abstract
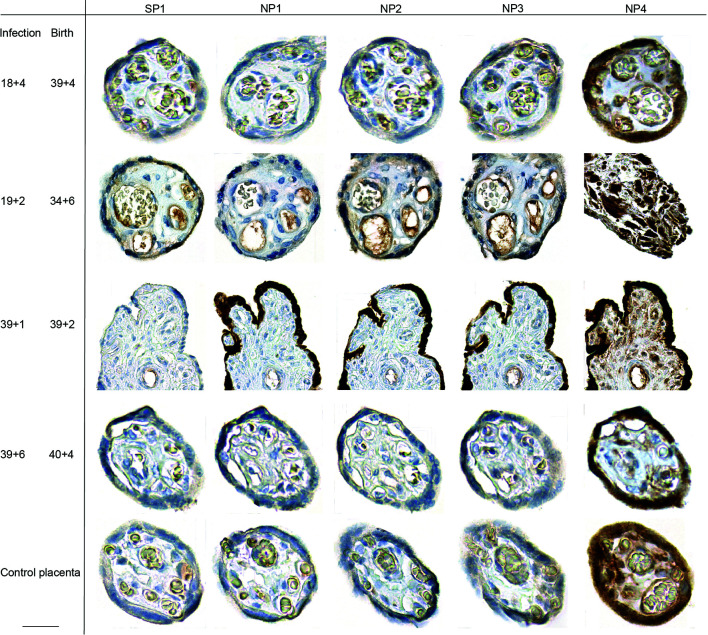
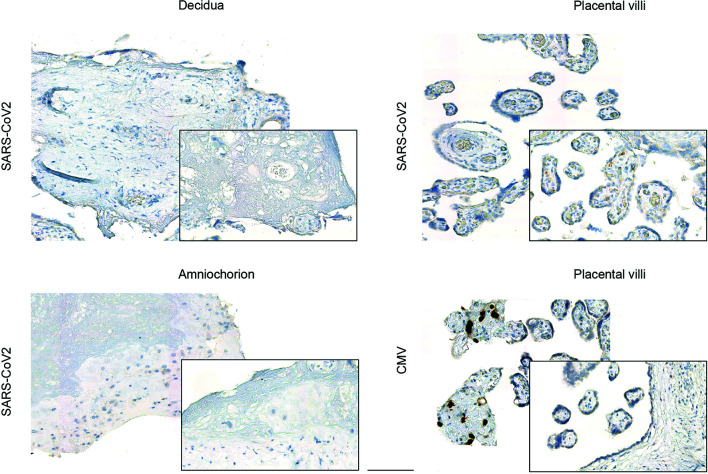
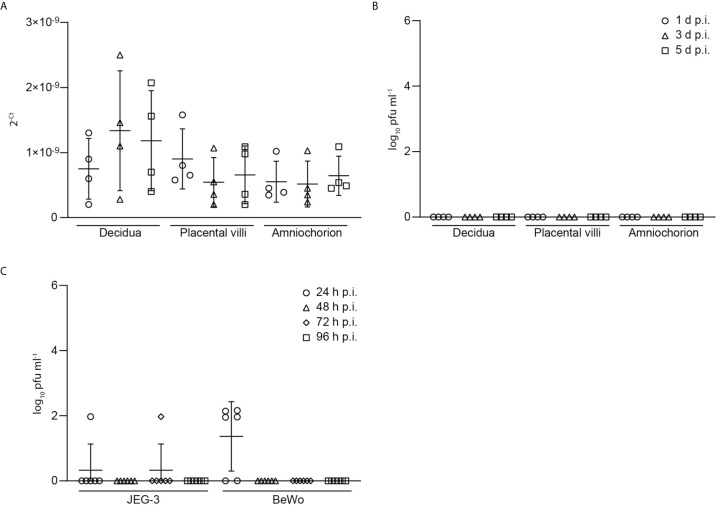
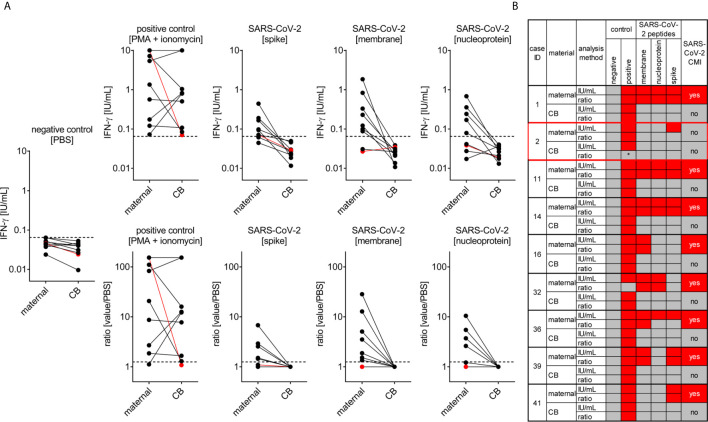
Pregnant women have been carefully observed during the COVID-19 pandemic, as the pregnancy-specific immune adaptation is known to increase the risk for infections. Recent evidence indicates that even though most pregnant have a mild or asymptomatic course, a severe course of COVID-19 and a higher risk of progression to diseases have also been described, along with a heightened risk for pregnancy complications. Yet, vertical transmission of the virus is rare and the possibility of placental SARS-CoV-2 infection as a prerequisite for vertical transmission requires further studies. We here assessed the severity of COVID-19 and onset of neonatal infections in an observational study of women infected with SARS-CoV-2 during pregnancy. Our placental analyses showed a paucity of SARS-CoV-2 viral expression ex vivo in term placentae under acute infection. No viral placental expression was detectable in convalescent pregnant women. Inoculation of placental explants generated from placentas of non-infected women at birth with SARS-CoV-2 in vitro revealed inefficient SARS-CoV-2 replication in different types of placental tissues, which provides a rationale for the low ex vivo viral expression. We further detected specific SARS-CoV-2 T cell responses in pregnant women within a few days upon infection, which was undetectable in cord blood. Our present findings confirm that vertical transmission of SARS-CoV-2 is rare, likely due to the inefficient virus replication in placental tissues. Despite the predominantly benign course of infection in most mothers and negligible risk of vertical transmission, continuous vigilance on the consequences of COVID-19 during pregnancy is required, since the maternal immune activation in response to the SARS-CoV2 infection may have long-term consequences for children's health.
Keywords: SARS-CoV; T cell response; human trial; prenatal infection; variants of concern; vertical transfer.
Copyright © 2021 Tallarek, Urbschat, Fonseca Brito, Stanelle-Bertram, Krasemann, Frascaroli, Thiele, Wieczorek, Felber, Lütgehetmann, Markert, Hecher, Brune, Stahl, Gabriel, Diemert and Arck.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Harris J. Influenza Occuring in Pregnant Women: A Statistical Study of Thirteen Hundred and Fifty Cases. JAMA (2019) 72(14):978–80. 10.1001/jama.1919.02610140008002 - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous