

Foveal regeneration after resolution of cystoid macular edema without and with internal limiting membrane detachment: presumed role of glial cells for foveal structure stabilization
- PMID: 34150536
- PMCID: PMC8165612
- DOI: 10.18240/ijo.2021.06.06
Foveal regeneration after resolution of cystoid macular edema without and with internal limiting membrane detachment: presumed role of glial cells for foveal structure stabilization
Abstract
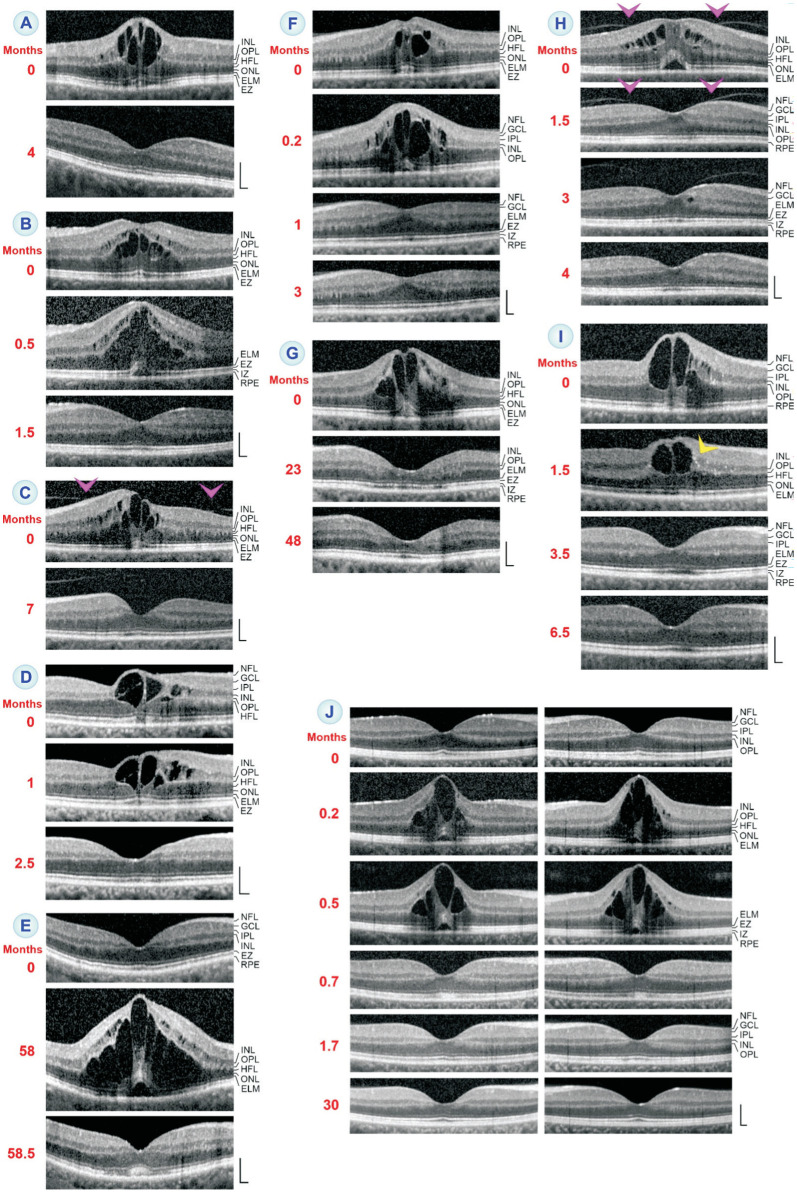
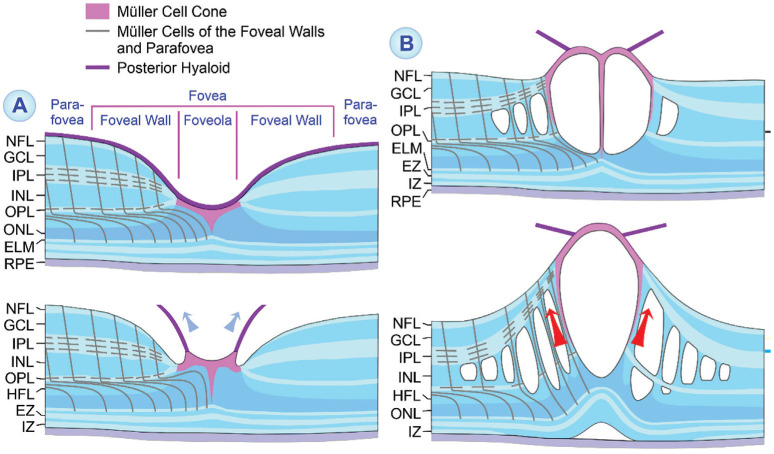
Aim: To document with spectral-domain optical coherence tomography the morphological regeneration of the fovea after resolution of cystoid macular edema (CME) without and with internal limiting membrane (ILM) detachment and to discuss the presumed role of the glial scaffold for foveal structure stabilization.
Methods: A retrospective case series of 38 eyes of 35 patients is described. Of these, 17 eyes of 16 patients displayed foveal regeneration after resolution of CME, and 6 eyes of 6 patients displayed CME with ILM detachment. Eleven eyes of 9 patients displayed other kinds of foveal and retinal disorders associated with ILM detachment.
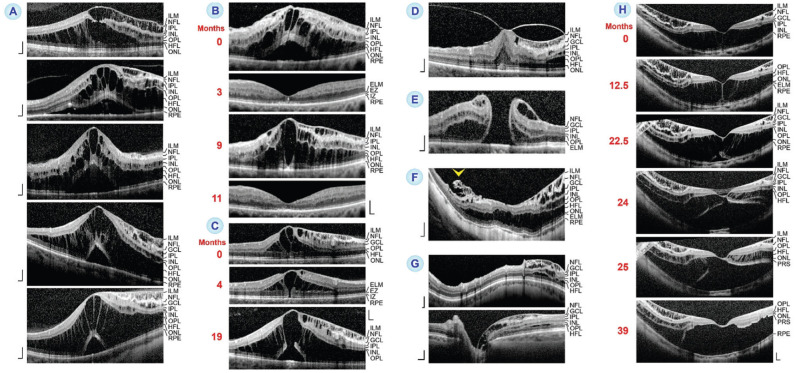
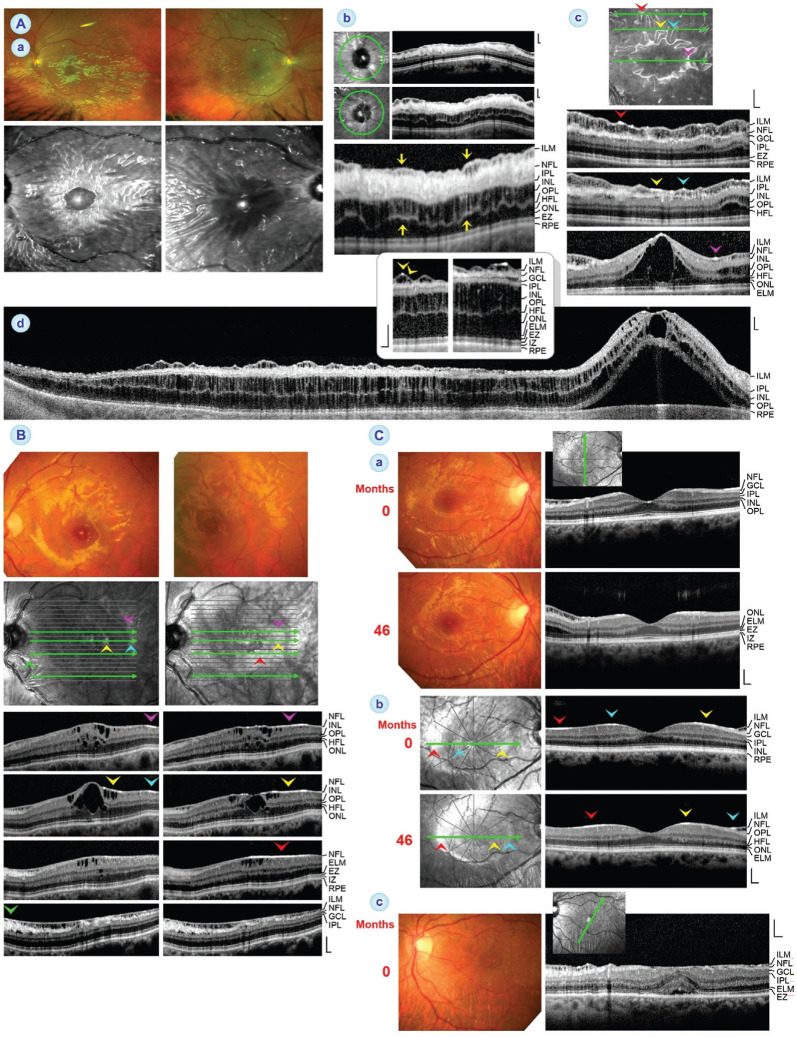
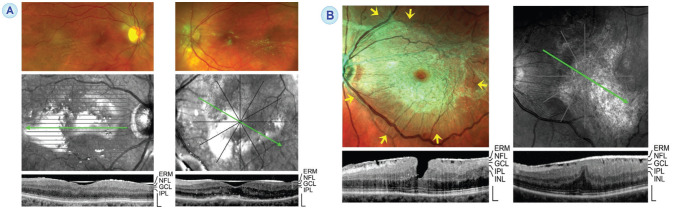
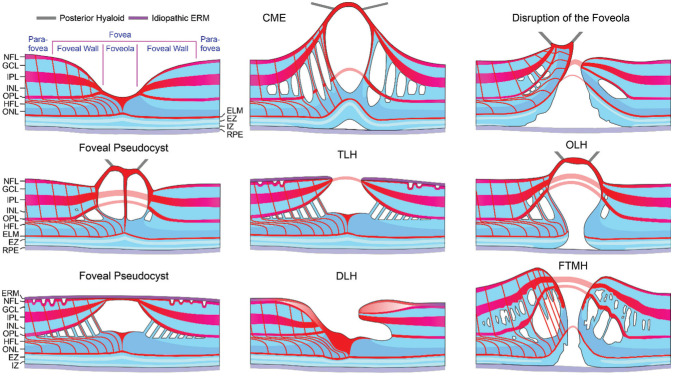
Results: The pattern of edematous cyst distribution, with or without a large cyst in the foveola and preferred location of cysts in the inner nuclear layer or Henle fiber layer (HFL), may vary between different eyes with CME or in one eye during different CME episodes. Large cysts in the foveola may be associated with a tractional elevation of the inner foveal layers and the formation of a foveoschisis in the HFL. Edematous cysts are usually not formed in the ganglion cell layer. Eyes with CME and ILM detachment display a schisis between the detached ILM and nerve fiber layer (NFL) which is traversed by Müller cell trunks. ILM detachment was also found in single eyes with myopic traction maculopathy, macular pucker, full-thickness macular holes, outer lamellar holes, and glaucomatous parapapillary retinoschisis, and in 3 eyes with Müller cell sheen dystrophy (MCSD). As observed in eyes with MCSD, cellophane maculopathy, and macular pucker, respectively, fundus light reflections can be caused by different highly reflective membranes or layers: the thickened and tightened ILM which may or may not be detached from the NFL, the NFL, or idiopathic epiretinal membranes. In eyes with short single or multiple CME episodes, the central fovea regenerated either completely, which included the disappearance of irregularities of the photoreceptor layer lines and the reformation of a fovea externa, or with remaining irregularities of the photoreceptor layer lines.
Conclusion: The examples of a complete regeneration of the foveal morphology after transient CME show that the fovea may withstand even large tractional deformations and has a conspicuous capacity of structural regeneration as long as no cell degeneration occurs. It is suggested that the regenerative capacity depends on the integrity of the threedimensional glial scaffold for foveal structure stabilization composed of Müller cell and astrocyte processes. The glial scaffold may also maintain the retinal structure after loss of most retinal neurons as in late-stage MCSD.
Keywords: Müller cell sheen dystrophy; Müller glia; astrocytes; cystoid macular edema; fovea; internal limiting membrane detachment.
International Journal of Ophthalmology Press.
Figures

Similar articles
-
Müller cells and astrocytes in tractional macular disorders.Prog Retin Eye Res. 2022 Jan;86:100977. doi: 10.1016/j.preteyeres.2021.100977. Epub 2021 Jun 5. Prog Retin Eye Res. 2022. PMID: 34102317 Review.
-
Morphology of partial-thickness macular defects: presumed roles of Müller cells and tissue layer interfaces of low mechanical stability.Int J Retina Vitreous. 2020 Jul 6;6:28. doi: 10.1186/s40942-020-00232-1. eCollection 2020. Int J Retina Vitreous. 2020. PMID: 32647586 Free PMC article.
-
Foveal configurations with disappearance of the foveal pit in eyes with macular pucker: Presumed role of Müller cells in the formation of foveal herniation.Exp Eye Res. 2021 Jun;207:108604. doi: 10.1016/j.exer.2021.108604. Epub 2021 Apr 27. Exp Eye Res. 2021. PMID: 33930399
-
Degenerative lamellar macular holes: tractional development and morphological alterations.Int Ophthalmol. 2021 Apr;41(4):1203-1221. doi: 10.1007/s10792-020-01674-0. Epub 2021 Jan 12. Int Ophthalmol. 2021. PMID: 33433772 Free PMC article.
-
The primate fovea: Structure, function and development.Prog Retin Eye Res. 2018 Sep;66:49-84. doi: 10.1016/j.preteyeres.2018.03.006. Epub 2018 Mar 30. Prog Retin Eye Res. 2018. PMID: 29609042 Review.
Cited by
-
Sustained Retinal Defocus Increases the Effect of Induced Myopia on the Retinal Astrocyte Template.Cells. 2024 Mar 29;13(7):595. doi: 10.3390/cells13070595. Cells. 2024. PMID: 38607034 Free PMC article.
-
Assessment of the Retinal Ganglion Cell Layer after Uncomplicated Cataract Surgery.J Clin Med. 2024 Jun 19;13(12):3579. doi: 10.3390/jcm13123579. J Clin Med. 2024. PMID: 38930108 Free PMC article.
-
Retinal Vascularity in Military Pilots in Relation to the Type of Aircraft, Flight Altitude and Total Hours of Flight.J Clin Med. 2025 Apr 14;14(8):2671. doi: 10.3390/jcm14082671. J Clin Med. 2025. PMID: 40283501 Free PMC article.
-
The Role of Müller Cells in Diabetic Macular Edema.Invest Ophthalmol Vis Sci. 2023 Jul 3;64(10):8. doi: 10.1167/iovs.64.10.8. Invest Ophthalmol Vis Sci. 2023. PMID: 37418272 Free PMC article. Review.
-
Morphology of foveal hypoplasia: Hyporeflective zones in the Henle fiber layer of eyes with high-grade foveal hypoplasia.PLoS One. 2022 Apr 13;17(4):e0266968. doi: 10.1371/journal.pone.0266968. eCollection 2022. PLoS One. 2022. PMID: 35417487 Free PMC article.
References
-
- Bringmann A, Syrbe S, Görner K, Kacza J, Francke M, Wiedemann P, Reichenbach A. The primate fovea: structure, function and development. Prog Retin Eye Res. 2018;66:49–84. - PubMed
-
- Reichenbach A, Hagen E, Schippel K, Eberhardt W. Quantitative electron microscopy of rabbit Müller (glial) cells in dependence on retinal topography. Z Mikrosk Anat Forsch. 1988;102(5):721–755. - PubMed
-
- Holländer H, Makarov F, Dreher Z, van Driel D, Chan-Ling TL, Stone J. Structure of the macroglia of the retina: sharing and division of labour between astrocytes and Müller cells. J Comp Neurol. 1991;313(4):587–603. - PubMed
-
- Yamada E. Some structural features of the fovea centralis in the human retina. Arch Ophthalmol. 1969;82(2):151–159. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials