

Surgical outcomes in acute dacryocystitis patients undergoing endonasal endoscopic dacryocystorhinostomy with or without silicone tube intubation
- PMID: 34150538
- PMCID: PMC8165628
- DOI: 10.18240/ijo.2021.06.08
Surgical outcomes in acute dacryocystitis patients undergoing endonasal endoscopic dacryocystorhinostomy with or without silicone tube intubation
Abstract
Aim: To establish the necessity of silicone tube intubation in acute dacryocystitis (AD) patients undergoing endonasal endoscopic dacryocystorhinostomy (En-DCR).
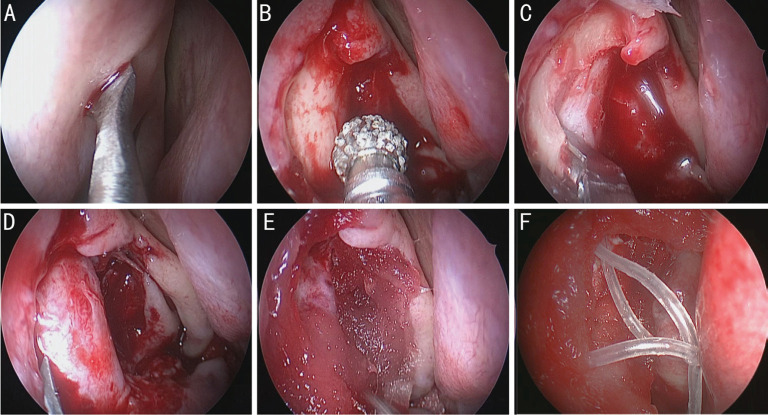
Methods: Patients presenting with unilateral AD were randomly assigned to two treatment groups. En-DCR procedures were performed following lacrimal abscess formation, with the operation being performed with silicone intubation for patients in group B but not group A. Functional success was defined by an absence of additional AD episodes, no epiphora, and ostium patency as established via endoscopic evaluation or fluorescein irrigation. Operative success rates and demographic variables were compared between treatment groups.
Results: In total, 66 patients were analyzed in the present study (33 per group), with complete postoperative data having been successfully collected from 27 and 22 patients in group A and group B, respectively. All patients exhibited complete resolution of acute inflammation. Upon follow-up, granulation tissue was detected around the ostium at higher rates in group B (9/22, 40.9%) relative to group A (4/27, 14.8%). At the 12-month follow-up time point, patients in group A exhibited higher success rates (25/27, 92.6%) relative to patients in group B (20/22, 90.9%), but this difference was not significant. Cases of lacrimal passage reconstruction failure in both groups were attributed to excessive fibrous and/or granulation tissue formation proximal to the intranasal ostium.
Conclusion: Given that these two operative approaches are associated with similar rates of operative success and in light of differences in granulation tissue formation, cost, and operative duration, these data do not support the routine silicone intubation of AD patients following En-DCR surgery.
Keywords: En-DCR; acute dacryocystitis; granulation; silicone tube.
International Journal of Ophthalmology Press.
Figures




References
-
- Ali MJ, Joshi SD, Naik MN, Honavar SG. Clinical profile and management outcome of acute dacryocystitis: two decades of experience in a tertiary eye care center. Semin Ophthalmol. 2015;30(2):118–123. - PubMed
-
- Cahill KV, Burns JA. Management of acute dacryocystitis in adults. Ophthalmic Plast Reconstr Surg. 1993;9(1):38–41. - PubMed
-
- Huber-Spitzy V, Steinkogler FJ, Huber E, Arocker-Mettinger E, Schiffbänker M. Acquired dacryocystitis: microbiology and conservative therapy. Acta Ophthalmol (Copenh) 1992;70(6):745–749. - PubMed
-
- Coden DJ, Hornblass A, Haas BD. Clinical bacteriology of dacryocystitis in adults. Ophthalmic Plast Reconstr Surg. 1993;9(2):125–131. - PubMed
-
- Lee TS, Woog JJ. Endonasal dacryocystorhinostomy in the primary treatment of acute dacryocystitis with abscess formation. Ophthalmic Plast Reconstr Surg. 2001;17(3):180–183. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials