

Dietary Salt Reduction, Prevalence of Hypertension and Avoidable Burden of Stroke in Vietnam: Modelling the Health and Economic Impacts
- PMID: 34150712
- PMCID: PMC8213032
- DOI: 10.3389/fpubh.2021.682975
Dietary Salt Reduction, Prevalence of Hypertension and Avoidable Burden of Stroke in Vietnam: Modelling the Health and Economic Impacts
Abstract
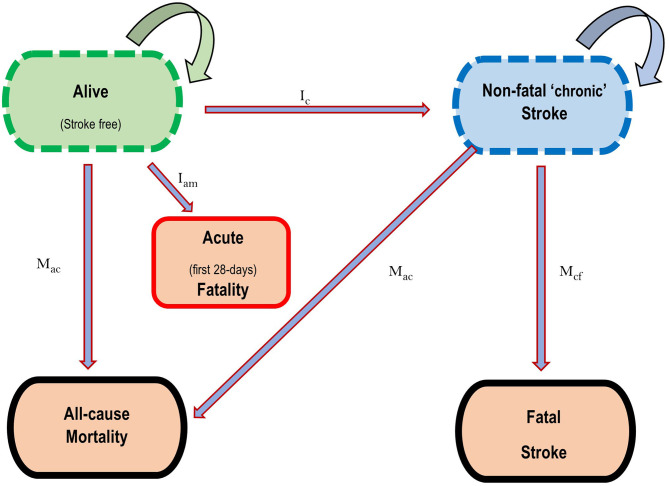
Dietary salt reduction has been recommended as a cost-effective population-wide strategy to prevent cardiovascular disease. The health and economic impact of salt consumption on the future burden of stroke in Vietnam is not known. Objective: To estimate the avoidable incidence of and deaths from stroke, as well as the healthy life years and healthcare costs that could be gained from reducing salt consumption in Vietnam. Methods: This was a macrosimulation health and economic impact assessment study. Data on blood pressure, salt consumption and stroke epidemiology were obtained from the Vietnam 2015 STEPS survey and the Global Burden of Disease study. A proportional multi-cohort multistate lifetable Markov model was used to estimate the impact of achieving the Vietnam national salt targets of 8 g/day by 2025 and 7 g/day by 2030, and to the 5 g/day WHO recommendation by 2030. Probabilistic sensitivity analysis was conducted to quantify the uncertainty in our projections. Results: If the 8 g/day, 7 g/day, and 5 g/day targets were achieved, the prevalence of hypertension could reduce by 1.2% (95% uncertainty interval [UI]: 0.5 to 2.3), 2.0% (95% UI: 0.8 to 3.6), and 3.5% (95% UI: 1.5 to 6.3), respectively. This would translate, respectively, to over 80,000, 180,000, and 257,000 incident strokes and over 18,000, 55,000, and 73,000 stroke deaths averted. By 2025, over 56,554 stroke-related health-adjusted life years (HALYs) could be gained while saving over US$ 42.6 million in stroke healthcare costs. By 2030, about 206,030 HALYs (for 7 g/day target) and 262,170 HALYs (for 5 g/day target) could be gained while saving over US$ 88.1 million and US$ 122.3 million in stroke healthcare costs respectively. Conclusion: Achieving the national salt reduction targets could result in substantial population health and economic benefits. Estimated gains were larger if the WHO salt targets were attained and if changes can be sustained over the longer term. Future work should consider the equity impacts of specific salt reduction programs.
Keywords: blood pressure; healthcare costs; mortality; multi-state model; sodium; stroke.
Copyright © 2021 Aminde, Phung, Phung, Cobiac and Veerman.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



Similar articles
-
Avoidable burden of stomach cancer and potential gains in healthy life years from gradual reductions in salt consumption in Vietnam, 2019-2030: a modelling study.Public Health Nutr. 2023 Mar;26(3):586-597. doi: 10.1017/S136898002200177X. Epub 2022 Aug 19. Public Health Nutr. 2023. PMID: 35983611 Free PMC article.
-
Potential impact of a modest reduction in salt intake on blood pressure, cardiovascular disease burden and premature mortality: a modelling study.Open Heart. 2019 Feb 14;6(1):e000943. doi: 10.1136/openhrt-2018-000943. eCollection 2019. Open Heart. 2019. PMID: 30997132 Free PMC article.
-
Cost-effectiveness analysis of low-sodium potassium-rich salt substitutes in Indonesia: an equity modelling study.Lancet Reg Health Southeast Asia. 2024 Jun 13;26:100432. doi: 10.1016/j.lansea.2024.100432. eCollection 2024 Jul. Lancet Reg Health Southeast Asia. 2024. PMID: 39081840 Free PMC article.
-
Impact of Salt Intake on the Pathogenesis and Treatment of Hypertension.Adv Exp Med Biol. 2017;956:61-84. doi: 10.1007/5584_2016_147. Adv Exp Med Biol. 2017. PMID: 27757935 Review.
-
[Salt consumption and cerebrovascular diseases].Acta Med Croatica. 2010 May;64(2):123-8. Acta Med Croatica. 2010. PMID: 20649078 Review. Croatian.
Cited by
-
Public health economic modelling in evaluations of salt and/or alcohol policies: a systematic scoping review.BMC Public Health. 2025 Jan 8;25(1):82. doi: 10.1186/s12889-024-21237-7. BMC Public Health. 2025. PMID: 39780075 Free PMC article.
-
Comprehensive analysis of stroke epidemiology in Vietnam: Insights from GBD 1990-2019 and RES-Q 2017-2023.Glob Epidemiol. 2025 Apr 10;9:100199. doi: 10.1016/j.gloepi.2025.100199. eCollection 2025 Jun. Glob Epidemiol. 2025. PMID: 40276373 Free PMC article.
-
Cost-effectiveness of non-communicable disease prevention in Southeast Asia: a scoping review.Front Public Health. 2023 Nov 9;11:1206213. doi: 10.3389/fpubh.2023.1206213. eCollection 2023. Front Public Health. 2023. PMID: 38026322 Free PMC article.
-
Pattern of salt intake among Iranian hypertensive patients: insights from the 2021 STEPS study.J Diabetes Metab Disord. 2025 Jun 7;24(1):142. doi: 10.1007/s40200-025-01649-x. eCollection 2025 Jun. J Diabetes Metab Disord. 2025. PMID: 40491692
-
Reduction of Cardiovascular Events and Related Healthcare Expenditures through Achieving Population-Level Targets of Dietary Salt Intake in Japan: A Simulation Model Based on the National Health and Nutrition Survey.Nutrients. 2022 Aug 31;14(17):3606. doi: 10.3390/nu14173606. Nutrients. 2022. PMID: 36079865 Free PMC article.
References
-
- Ministry of Health General Department of Preventive Medicine . National Survey on the Risk Factors of Non-Communicable Diseases (STEPS). Vietnam (2015).
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical