

Sodium-Glucose Co-transporter-2 Inhibitors and Nephroprotection in Diabetic Patients: More Than a Challenge
- PMID: 34150796
- PMCID: PMC8212983
- DOI: 10.3389/fmed.2021.654557
Sodium-Glucose Co-transporter-2 Inhibitors and Nephroprotection in Diabetic Patients: More Than a Challenge
Abstract
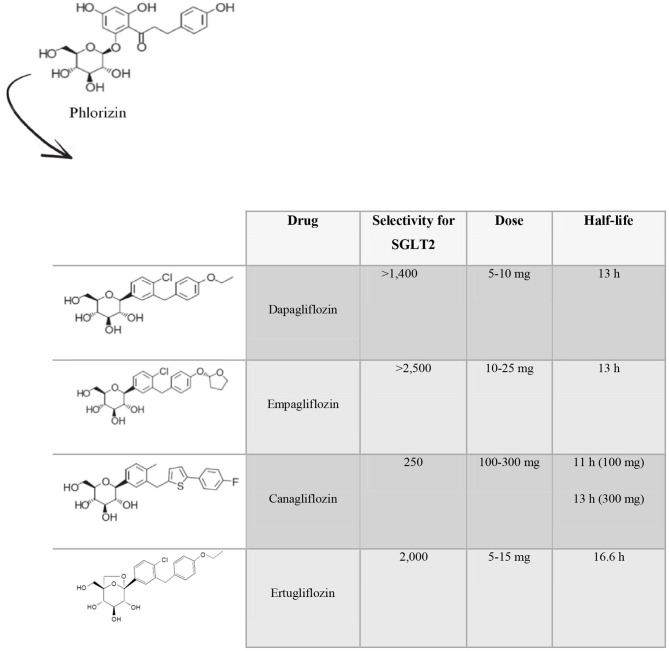
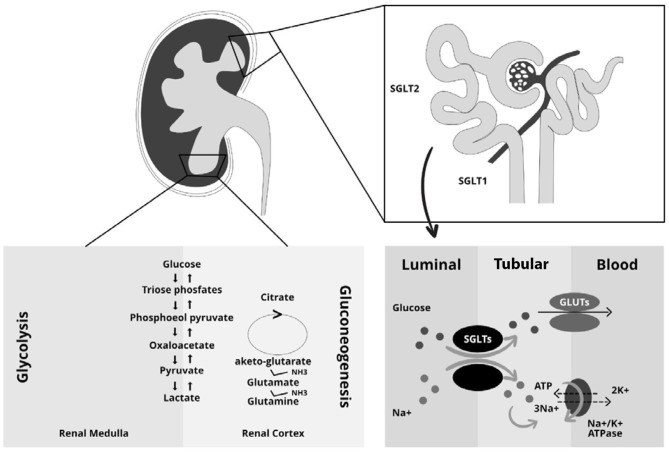
Diabetic nephropathy is the most common cause of end-stage renal disease worldwide. Control of blood glucose and blood pressure (BP) reduces the risk of developing this complication, but once diabetic nephropathy is established, it is then only possible to slow its progression. Sodium-glucose cotransporter-2 inhibitors (SGLT2is) are a novel class of oral hypoglycemic agents that increase urinary glucose excretion by suppressing glucose reabsorption at the renal proximal tubule. SGLT2is lower glycated hemoglobin (HbA1c) without increasing the risk of hypoglycemia, induce weight loss and improve various metabolic parameters including BP, lipid profile, albuminuria and uric acid. Several clinical trials have shown that SGLT2is (empagliflozin, dapagliflozin canagliflozin, and ertugliflozin) improve cardiovascular and renal outcomes and mortality in patients with type 2 diabetes. Effects of SGLT2is on the kidney can be explained by multiple pathways. SGLT2is may improve renal oxygenation and intra-renal inflammation thereby slowing the progression of kidney function decline. Additionally, SGLT2is are associated with a reduction in glomerular hyperfiltration, an effect which is mediated by the increase in natriuresis, the re-activation of tubule-glomerular feedback and independent of glycemic control. In this review, we will focus on renal results of major cardiovascular and renal outcome trials and we will describe direct and indirect mechanisms through which SGLT2is confer renal protection.
Keywords: CKD; SGLT2i; cardiovascular risk; clinical trials; renal risk; review; type 2 diabetes.
Copyright © 2021 Provenzano, Pelle, Zaffina, Tassone, Pujia, Ricchio, Serra, Sciacqua, Michael, Andreucci and Arturi.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Chronic Kidney Disease Prognosis Consortium. Matsushita K, van der Velde M, Astor BC, Woodward M, Levey AS, et al. . Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: a collaborative meta-analysis. Lancet. (2010) 375:2073–81. 10.1016/S0140-6736(10)60674-5 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources