

Association between the nasopharyngeal microbiome and metabolome in patients with COVID-19
- PMID: 34151035
- PMCID: PMC8200311
- DOI: 10.1016/j.synbio.2021.06.002
Association between the nasopharyngeal microbiome and metabolome in patients with COVID-19
Abstract
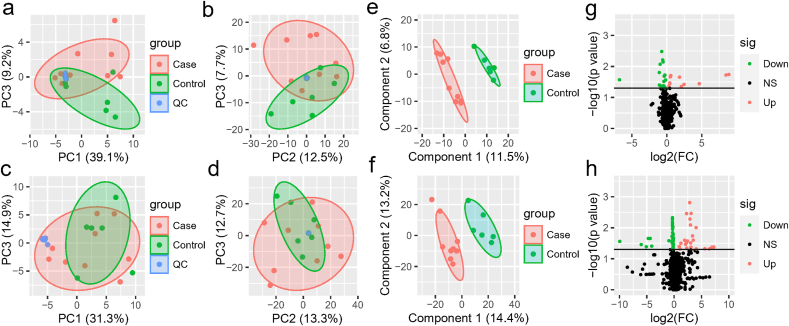
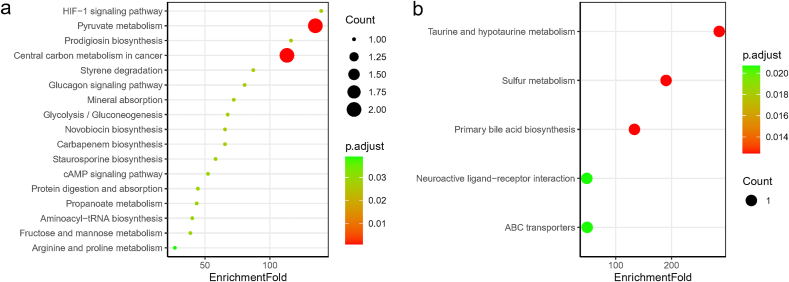
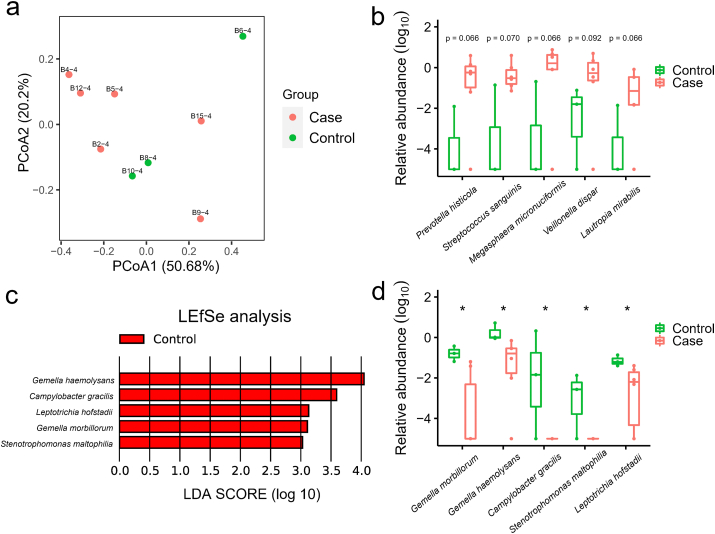
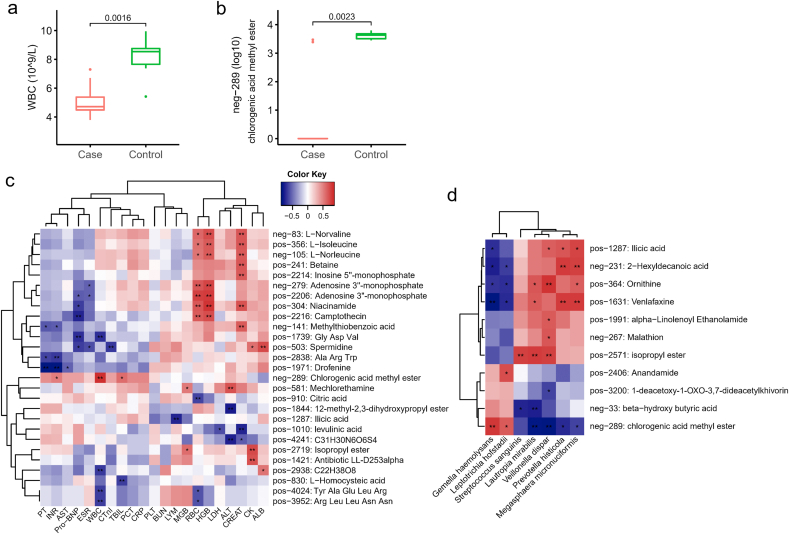
SARS-CoV-2, the causative agent for COVID-19, infect human mainly via respiratory tract, which is heavily inhabited by local microbiota. However, the interaction between SARS-CoV-2 and nasopharyngeal microbiota, and the association with metabolome has not been well characterized. Here, metabolomic analysis of blood, urine, and nasopharyngeal swabs from a group of COVID-19 and non-COVID-19 patients, and metagenomic analysis of pharyngeal samples were used to identify the key features of COVID-19. Results showed lactic acid, l-proline, and chlorogenic acid methyl ester (CME) were significantly reduced in the sera of COVID-19 patients compared with non-COVID-19 ones. Nasopharyngeal commensal bacteria including Gemella morbillorum, Gemella haemolysans and Leptotrichia hofstadii were notably depleted in the pharynges of COVID-19 patients, while Prevotella histicola, Streptococcus sanguinis, and Veillonella dispar were relatively increased. The abundance of G. haemolysans and L. hofstadii were significantly positively associated with serum CME, which might be an anti-SARS-CoV-2 bacterial metabolite. This study provides important information to explore the linkage between nasopharyngeal microbiota and disease susceptibility. The findings were based on a very limited number of patients enrolled in this study; a larger size of cohort will be appreciated for further investigation.
Keywords: COVID-19; Metabolome; Nasopharyngeal microbiome; SARS-CoV-2; Susceptibility.
© 2021 The Authors.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures

References
LinkOut - more resources
Full Text Sources
Miscellaneous
