

Impact of Pharmacologically Left Shifting the Oxygen-Hemoglobin Dissociation Curve on Arterial Blood Gases and Pulmonary Gas Exchange During Maximal Exercise in Hypoxia
- PMID: 34152867
- PMCID: PMC8665803
- DOI: 10.1089/ham.2020.0159
Impact of Pharmacologically Left Shifting the Oxygen-Hemoglobin Dissociation Curve on Arterial Blood Gases and Pulmonary Gas Exchange During Maximal Exercise in Hypoxia
Abstract
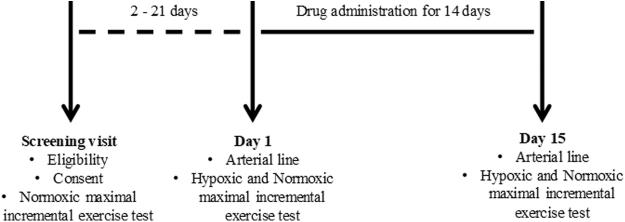
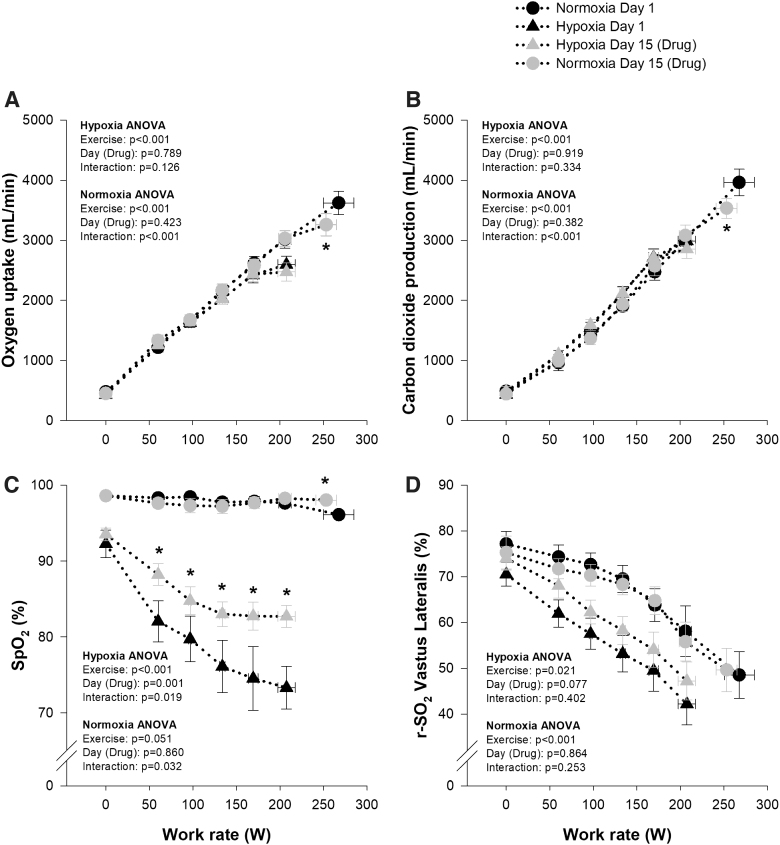
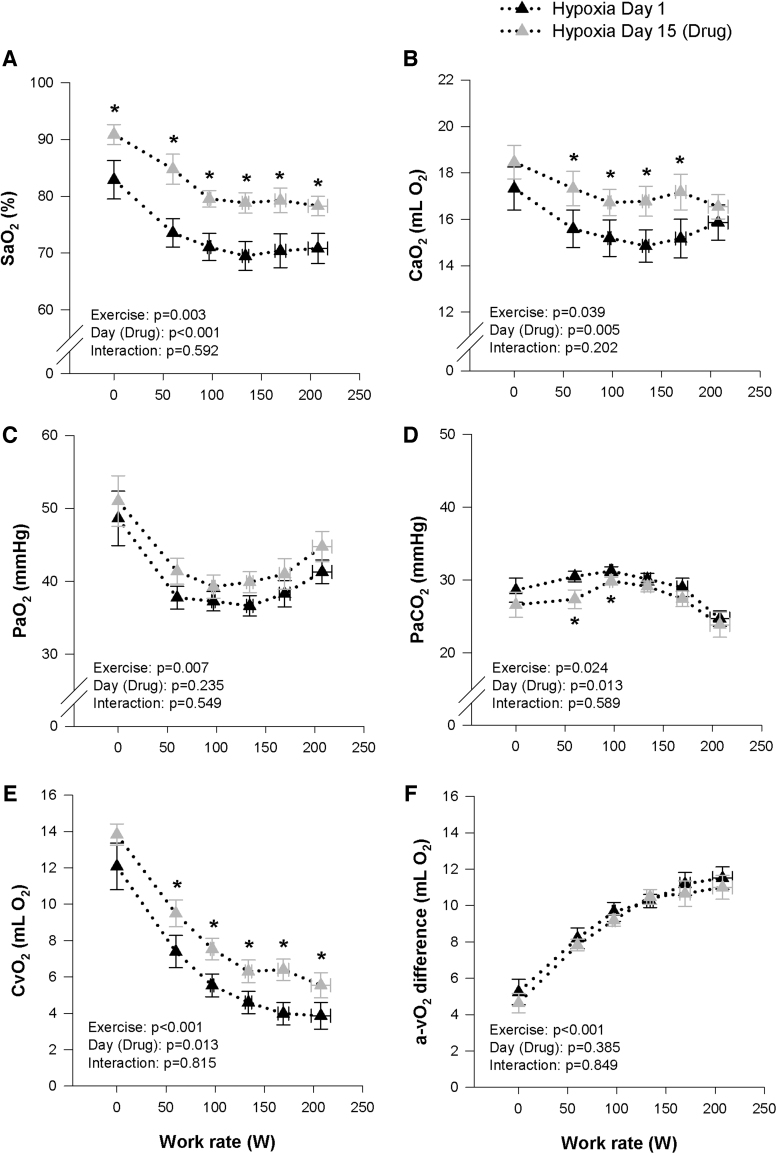
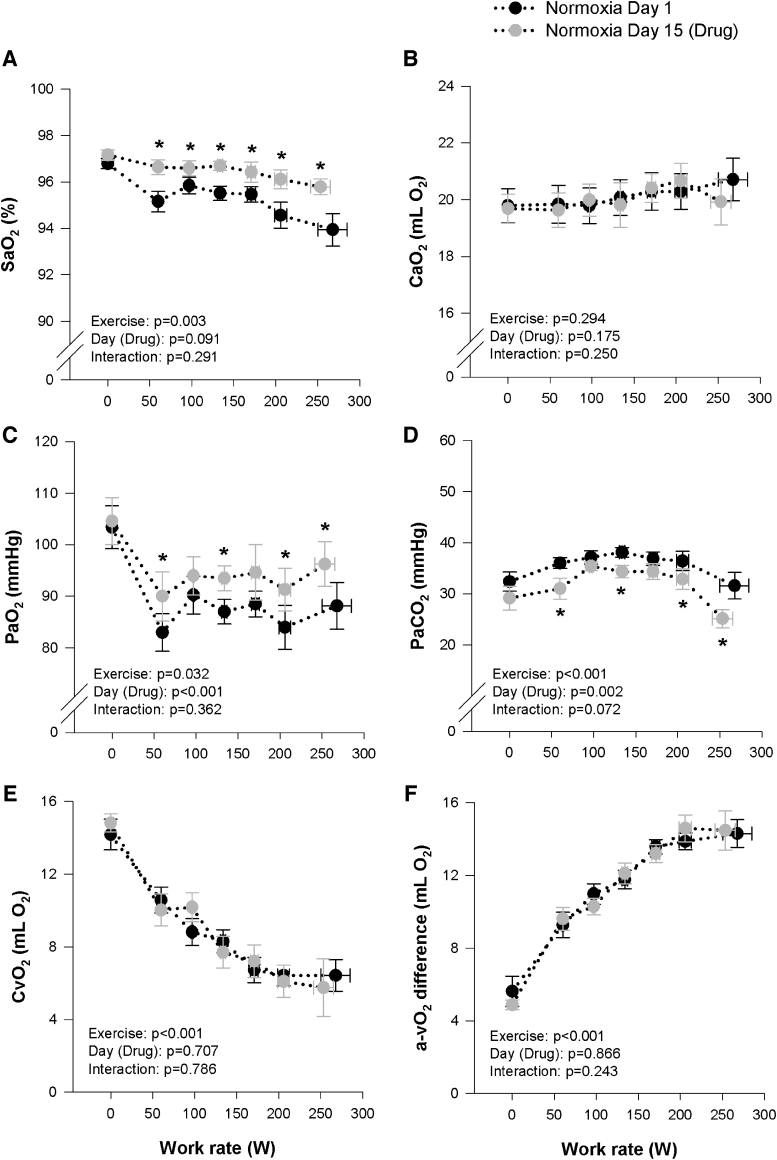
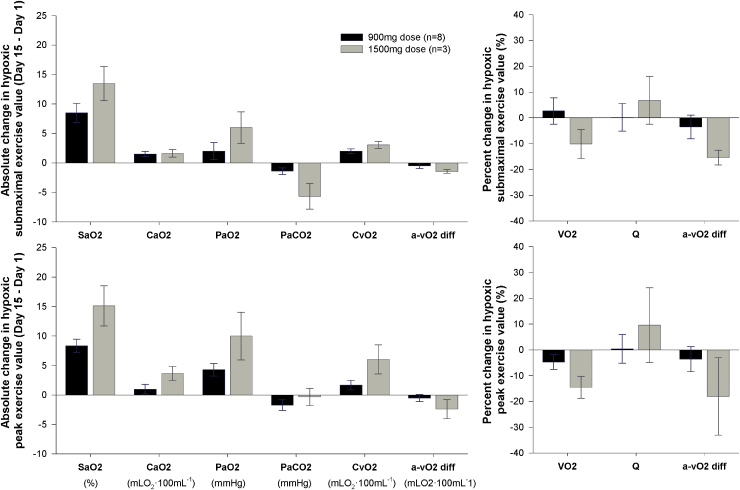
Stewart, Glenn M., Troy J. Cross, Michael J. Joyner, Steven C. Chase, Timothy Curry, Josh Lehrer-Graiwer, Kobina Dufu, Nicholas E. Vlahakis, and Bruce D. Johnson. Impact of pharmacologically left shifting the oxygen-hemoglobin dissociation curve on arterial blood gases and pulmonary gas exchange during maximal exercise in hypoxia. High Alt Med Biol. 22:249-262, 2021. Introduction: Physiological and pathological conditions, which reduce the loading of oxygen onto hemoglobin (Hb), can impair exercise capacity and cause debilitating symptoms. Accordingly, this study examined the impact of pharmacologically left shifting the oxygen-hemoglobin dissociation curve (ODC) on arterial oxygen saturation (SaO2) and exercise capacity. Methods: Eight healthy subjects completed a maximal incremental exercise test in hypoxia (FIO2: 0.125) and normoxia (FIO2: 0.21) before (Day 1) and after (Day 15) daily ingestion of 900 mg of voxelotor (an oxygen/Hb affinity modulator). Pulmonary gas exchange and arterial blood gases were assessed throughout exercise and at peak. Data for a 1,500 mg daily drug dose are reported in a limited cohort (n = 3). Results: Fourteen days of drug administration left shifted the ODC (p50 measured under standard conditions, Day 1: 28.0 ± 2.1 mmHg vs. Day 15: 26.1 ± 1.8 mmHg, p < 0.05). Throughout incremental exercise in hypoxia, SaO2 was systematically higher after drug (peak exercise SaO2 on Day 1: 71 ± 2 vs. Day 15: 81% ± 2%, p < 0.001), whereas oxygen extraction (Ca-vO2 diff) and consumption (VO2) were similar (peak exercise Ca-vO2 diff on Day 1: 11.5 ± 1.7 vs. Day 15: 11.0 ± 1.8 ml/100 ml blood, p = 0.417; peak VO2 on Day 1: 2.59 ± 0.39 vs. Day 15: 2.47 ± 0.43 l/min, p = 0.127). Throughout incremental exercise in normoxia, SaO2 was systematically higher after drug, whereas peak VO2 was reduced (peak exercise SaO2 on Day 1: 93.9 ± 1.8 vs. Day 15: 95.8% ± 1.0%, p = 0.008; peak VO2 on Day 1: 3.62 ± 0.55 vs. Day 15: 3.26 ± 52 l/min, p = 0.001). Conclusion: Pharmacologically increasing the affinity of Hb for oxygen improved SaO2 during hypoxia without impacting exercise capacity; however, left shifting the ODC in healthy individuals appears detrimental to exercise capacity in normoxia. Left shifting the ODC to different magnitudes and under more chronic forms of hypoxia warrants further study.
Keywords: GBT440; hematology; hypoxia; maximal oxygen uptake; oxygen affinity of hemoglobin; voxelotor.
Conflict of interest statement
The study was funded by Global Blood Therapeutics, and authors J.L.-G., K.D., and N.E.V. are employees of Global Blood Therapeutics.
Figures
References
-
- Adams RP, and Welch HG. (1980). Oxygen uptake, acid-base status, and performance with varied inspired oxygen fractions. J Appl Physiol Respir Environ Exerc Physiol 49:863–868. - PubMed
-
- Bell C, Monahan KD, Donato AJ, Hunt BE, Seals DR, and Beck KC. (2003). Use of acetylene breathing to determine cardiac output in young and older adults. Med Sci Sport Exer 35:58–64. - PubMed
-
- Calbet JA, Boushel R, Radegran G, Sondergaard H, Wagner PD, and Saltin B. (2003). Determinants of maximal oxygen uptake in severe acute hypoxia. Am J Physiol Regul Integr Comp Physiol 284:R291–303. - PubMed
-
- Calbet JA, Losa-Reyna J, Torres-Peralta R, Rasmussen P, Ponce-Gonzalez JG, Sheel AW, de la Calle-Herrero J, Guadalupe-Grau A, Morales-Alamo D, Fuentes T, Rodriguez-Garcia L, Siebenmann C, Boushel R, and Lundby C. (2015). Limitations to oxygen transport and utilization during sprint exercise in humans: Evidence for a functional reserve in muscle O2 diffusing capacity. J Physiol 593:4649–4664. - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
