

Melioidosis-a disease of socioeconomic disadvantage
- PMID: 34153059
- PMCID: PMC8248627
- DOI: 10.1371/journal.pntd.0009544
Melioidosis-a disease of socioeconomic disadvantage
Abstract
Background: There is growing recognition of the contribution of the social determinants of health to the burden of many infectious diseases. However, the relationship between socioeconomic status and the incidence and outcome of melioidosis is incompletely defined.
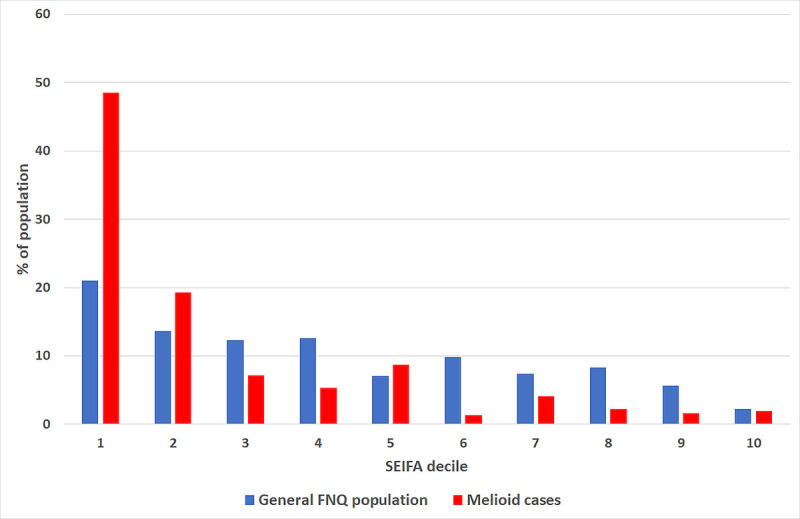
Methods: All residents of Far North Queensland, tropical Australia with culture-proven melioidosis between January 1998 and December 2020 were eligible for the study. Their demographics, comorbidities and socioeconomic status were correlated with their clinical course. Socioeconomic status was determined using the Socio-Economic Indexes for Areas (SEIFA) Index of Relative Socio-economic Disadvantage score, a measure of socioeconomic disadvantage developed by the Australian Bureau of Statistics. Socioeconomic disadvantage was defined as residence in a region with a SEIFA score in the lowest decile in Australia.
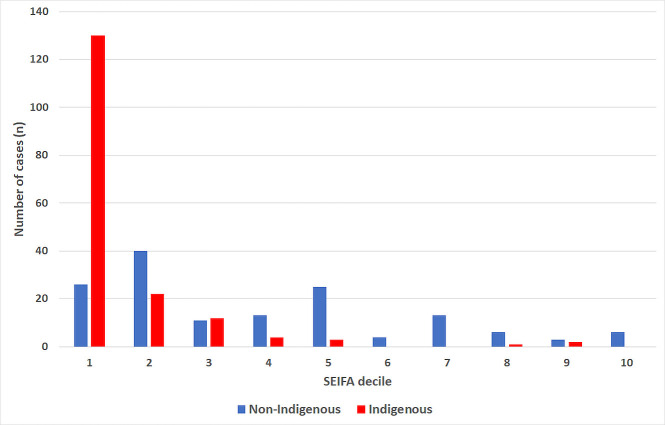
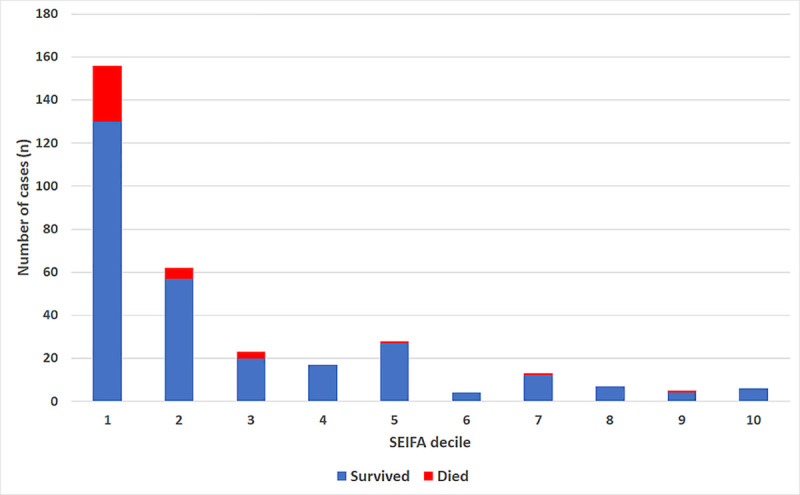
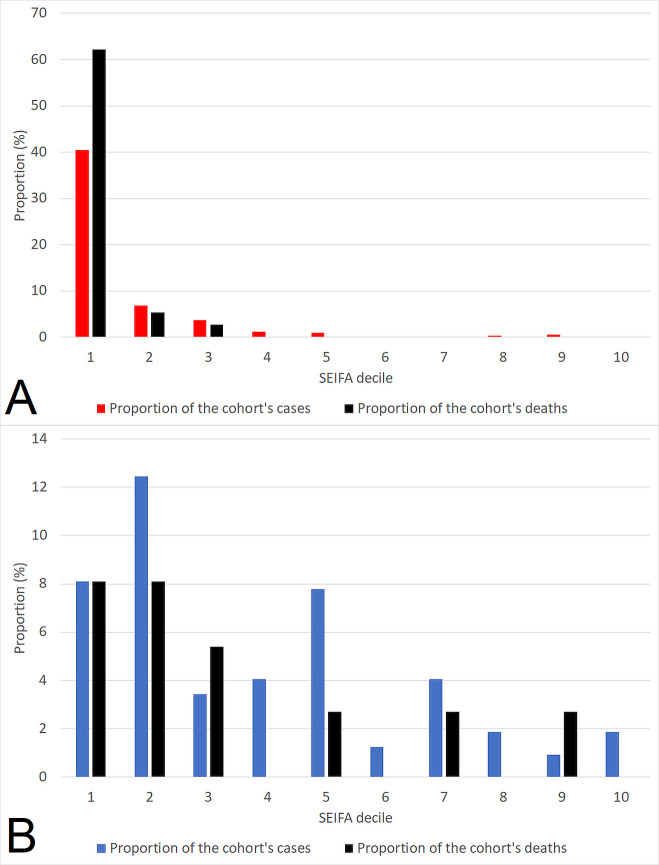
Results: 321 eligible individuals were diagnosed with melioidosis during the study period, 174 (54.2%) identified as Indigenous Australians; 223/321 (69.5%) were bacteraemic, 85/321 (26.5%) required Intensive Care Unit (ICU) admission and 37/321 (11.5%) died. 156/321 (48.6%) were socioeconomically disadvantaged, compared with 56603/269002 (21.0%) of the local general population (p<0.001). Socioeconomically disadvantaged patients were younger, more likely to be female, Indigenous, diabetic or have renal disease. They were also more likely to die prior to hospital discharge (26/156 (16.7%) versus 11/165 (6.7%), p = 0.002) and to die at a younger age (median (IQR) age: 50 (38-68) versus 65 (59-81) years, p = 0.02). In multivariate analysis that included age, Indigenous status, the presence of bacteraemia, ICU admission and the year of hospitalisation, only socioeconomic disadvantage (odds ratio (OR) (95% confidence interval (CI)): 2.49 (1.16-5.35), p = 0.02) and ICU admission (OR (95% CI): 4.79 (2.33-9.86), p<0.001) were independently associated with death.
Conclusion: Melioidosis is disease of socioeconomic disadvantage. A more holistic approach to the delivery of healthcare which addresses the social determinants of health is necessary to reduce the burden of this life-threatening disease.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Bossi P, Tegnell A, Baka A, Van Loock F, Hendriks J, Werner A, et al.. Bichat guidelines for the clinical management of glanders and melioidosis and bioterrorism-related glanders and melioidosis. Euro Surveill. 2004;9(12):E17–8. Epub 2005/01/29. . - PubMed
-
- Melioidosis; Bioterrorism: Centers for Disease Control and Prevention, National Center for Emerging and Zoonotic Infectious Diseases (NCEZID), Division of High-Consequence Pathogens and Pathology (DHCPP); 2017 [cited 2021 7 January]. Available from: https://www.cdc.gov/melioidosis/bioterrorism/index.html.
MeSH terms
LinkOut - more resources
Full Text Sources
