

Lung distribution of gas and blood volume in critically ill COVID-19 patients: a quantitative dual-energy computed tomography study
- PMID: 34154635
- PMCID: PMC8215486
- DOI: 10.1186/s13054-021-03610-9
Lung distribution of gas and blood volume in critically ill COVID-19 patients: a quantitative dual-energy computed tomography study
Abstract
Background: Critically ill COVID-19 patients have pathophysiological lung features characterized by perfusion abnormalities. However, to date no study has evaluated whether the changes in the distribution of pulmonary gas and blood volume are associated with the severity of gas-exchange impairment and the type of respiratory support (non-invasive versus invasive) in patients with severe COVID-19 pneumonia.
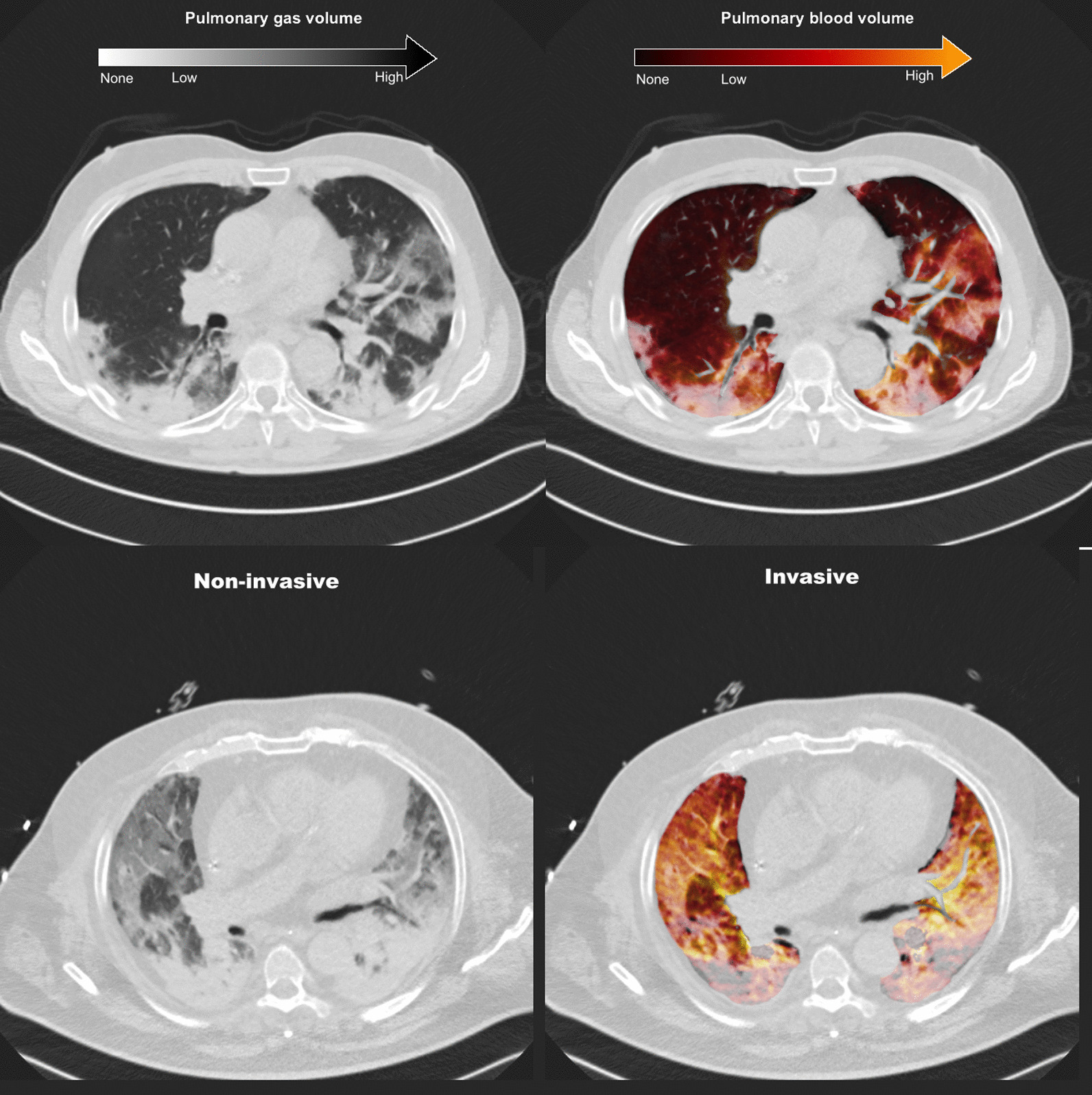
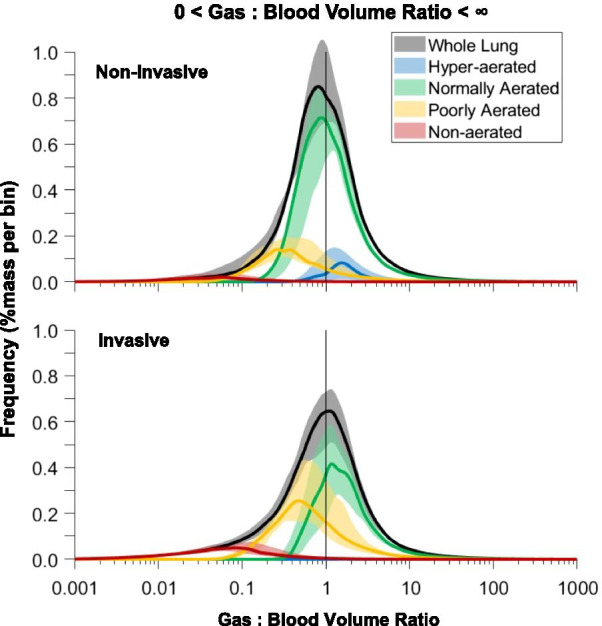
Methods: This was a single-center, retrospective cohort study conducted in a tertiary care hospital in Northern Italy during the first pandemic wave. Pulmonary gas and blood distribution was assessed using a technique for quantitative analysis of dual-energy computed tomography. Lung aeration loss (reflected by percentage of normally aerated lung tissue) and the extent of gas:blood volume mismatch (percentage of non-aerated, perfused lung tissue-shunt; aerated, non-perfused dead space; and non-aerated/non-perfused regions) were evaluated in critically ill COVID-19 patients with different clinical severity as reflected by the need for non-invasive or invasive respiratory support.
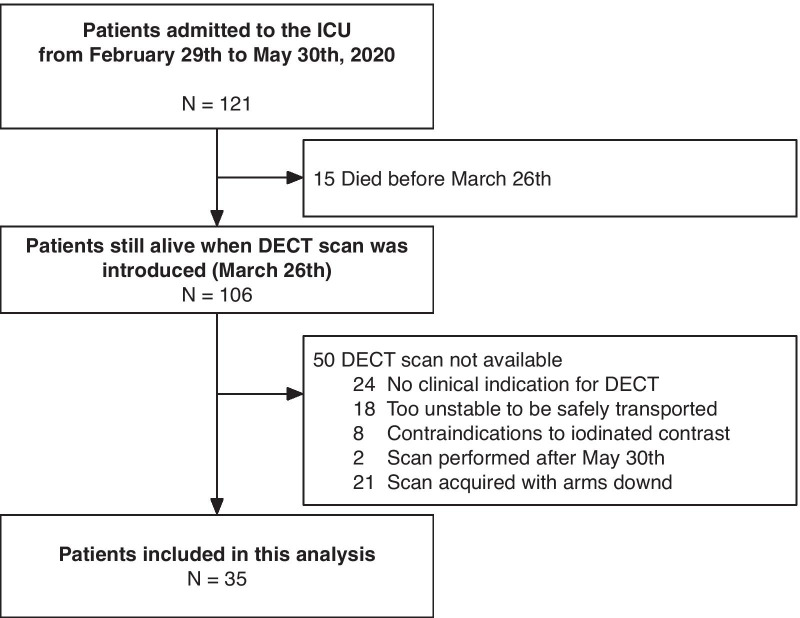
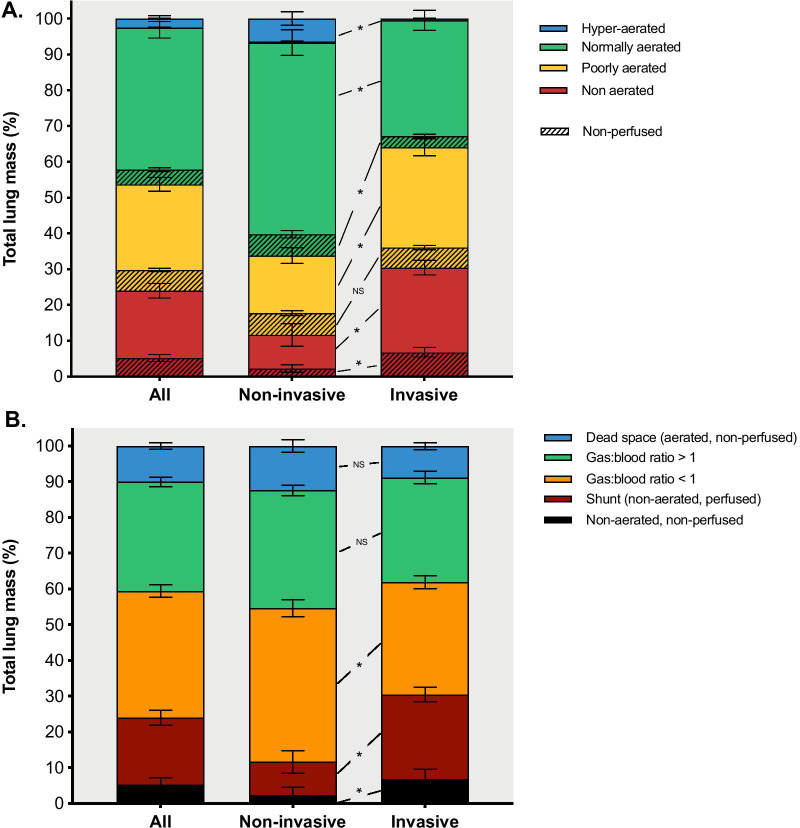
Results: Thirty-five patients admitted to the intensive care unit between February 29th and May 30th, 2020 were included. Patients requiring invasive versus non-invasive mechanical ventilation had both a lower percentage of normally aerated lung tissue (median [interquartile range] 33% [24-49%] vs. 63% [44-68%], p < 0.001); and a larger extent of gas:blood volume mismatch (43% [30-49%] vs. 25% [14-28%], p = 0.001), due to higher shunt (23% [15-32%] vs. 5% [2-16%], p = 0.001) and non-aerated/non perfused regions (5% [3-10%] vs. 1% [0-2%], p = 0.001). The PaO2/FiO2 ratio correlated positively with normally aerated tissue (ρ = 0.730, p < 0.001) and negatively with the extent of gas-blood volume mismatch (ρ = - 0.633, p < 0.001).
Conclusions: In critically ill patients with severe COVID-19 pneumonia, the need for invasive mechanical ventilation and oxygenation impairment were associated with loss of aeration and the extent of gas:blood volume mismatch.
Keywords: ARDS; COVID-19; Dual energy computed tomography; Lung imaging.
Conflict of interest statement
Dr. Bassetti reports personal fees and other from Angelini, personal fees and other from AstraZeneca, other from Bayer, personal fees and other from Cubist, personal fees and other from Pfizer, personal fees and other from Menarini, personal fees and other from MSD, other from Nabriva, other from Paratek, other from Roche, other from Shionogi, other from Tetraphase, other from The Medicine Company, personal fees and other from Astellas Pharma Inc., personal fees from Gilead Sciences, personal fees from Teva, personal fees from Novartis, grants from Ranbaxy, personal fees from Correvio, personal fees from Molteni, personal fees from Thermo Fisher, outside the submitted work. Dr. Herrmann is a cofounder and shareholder of OscillaVent, Inc, and consultant for ZOLL Medical Corporation, both outside the submitted work. Dr. Giacobbe reports personal fees from Stepstone Pharma GmbH, personal fees from MSD Italia, personal fees from Correvio Italia, outside the submitted work. Dr. Rocco reports personal fees from SANOFI as a DSMB member. All other authors declared no conflict of interest.
Figures

Comment in
-
The knowns and unknowns of perfusion disturbances in COVID-19 pneumonia.Crit Care. 2021 Sep 28;25(1):352. doi: 10.1186/s13054-021-03742-y. Crit Care. 2021. PMID: 34583761 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
