

Transarterial Chemoembolization in Treatment-Naïve and Recurrent Hepatocellular Carcinoma: A Propensity-Matched Outcome and Risk Signature Analysis
- PMID: 34155478
- PMCID: PMC8213527
- DOI: 10.3389/fonc.2021.662408
Transarterial Chemoembolization in Treatment-Naïve and Recurrent Hepatocellular Carcinoma: A Propensity-Matched Outcome and Risk Signature Analysis
Abstract
Objectives: The purpose of this study was to evaluate the efficacy and safety of transarterial chemoembolization (TACE) in the treatment of patients with treatment-naïve hepatocellular carcinoma (TN-HCC) and recurrent HCC (R-HCC). In addition, risk signature analysis was performed to accurately assess patients' recurrence and survival.
Methods: This retrospective study assessed the consecutive medical records of TN-HCC and R-HCC patients from January 2014 to December 2018. In order to reduce the patient selection bias, propensity score matching (PSM) analysis was applied. Conditional inference tree was used to establish a risk signature.
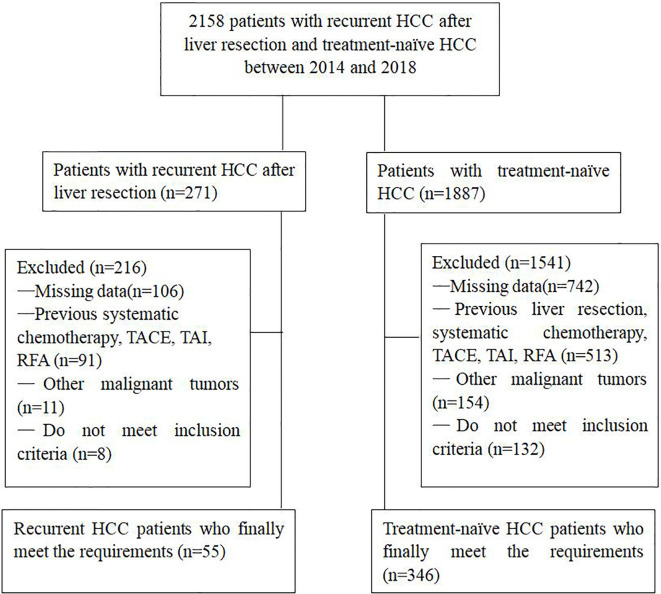
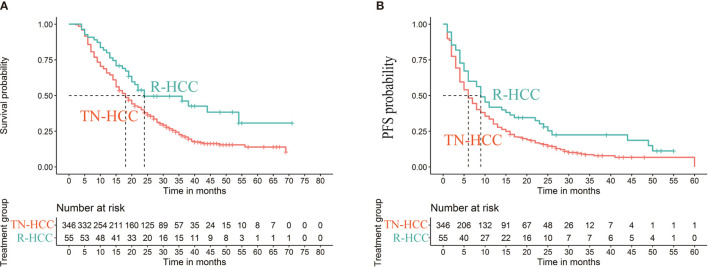
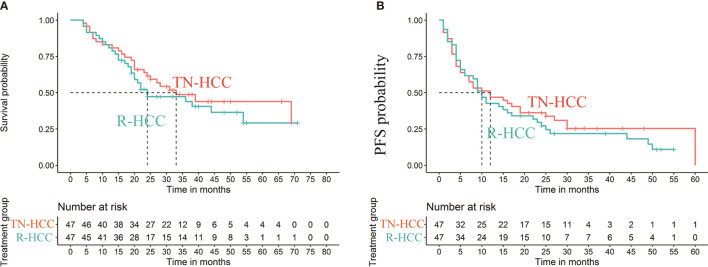
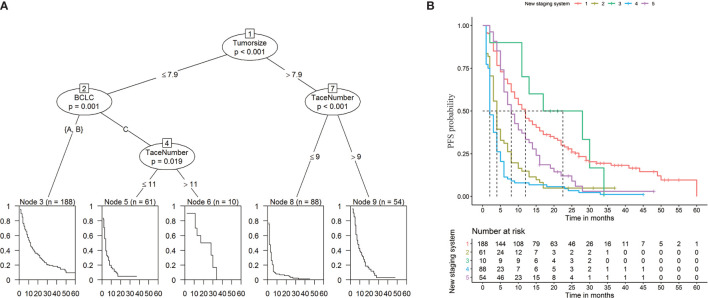
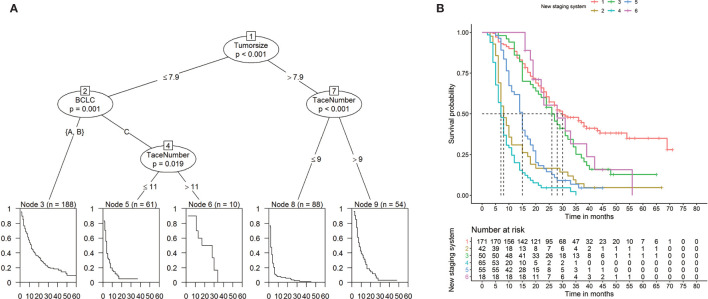
Results: A total of 401 eligible patients were included in our study, including 346 patients in the TN-HCC group and 55 patients in the R-HCC group. Forty-seven pairs of patients were chosen after the PSM analysis. Before the PSM analysis, the objective tumor regression (ORR) and disease control rate (DCR) of R-HCC patients were better than that of TN-HCC patients; however, after the PSM analysis, there was no significant difference in the ORR and DCR between the two groups (P>0.05). Before the PSM analysis, the median overall survival (OS) and progression-free survival (PFS) in the R-HCC group were significantly greater than those of the TN-HCC group (OS: 24 months vs. 18 months, P =0.004; PFS: 9 months vs. 6 months, P =0.012). However, after the PSM analysis, the median OS and PFS in the R-HCC group were inferior to those in the TN-HCC group (OS: 24 months vs. 33 months, P= 0.0035; PFS: 10 months vs. 12 months, P = 0.01). The conditional inference tree divided patients into different subgroups according to tumor size, BCLC stage, and TACE sessions and shared different hazards ratio to recurrence or survival.
Conclusion: Patients with R-HCC treated with TACE achieved satisfactory results, although survival after the PSM analysis was not as good as in the TN-HCC group. In addition, risk signature based on conditional inference tree analysis can more accurately predict the recurrence and survival in both groups of patients.
Keywords: hepatocellular carcinoma; liver resection; propensity score matching; recurrence; transarterial chemoembolization.
Copyright © 2021 Liu, Ren, Ge, Xiong, Zhou, Feng, Song and Zheng.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Comparison of DEB-TACE and cTACE for the initial treatment of unresectable hepatocellular carcinoma beyond up-to-seven criteria: A single-center propensity score matching analysis.Clin Res Hepatol Gastroenterol. 2022 May;46(5):101893. doi: 10.1016/j.clinre.2022.101893. Epub 2022 Mar 3. Clin Res Hepatol Gastroenterol. 2022. PMID: 35247625
-
Transarterial chemoembolization combined with apatinib with or without PD-1 inhibitors in BCLC stage C hepatocellular carcinoma: A multicenter retrospective study.Front Oncol. 2022 Sep 30;12:961394. doi: 10.3389/fonc.2022.961394. eCollection 2022. Front Oncol. 2022. PMID: 36249011 Free PMC article.
-
Transarterial chemoembolization combined with iodine 125 seeds versus transarterial chemoembolization combined with radiofrequency ablation in the treatment of early- and intermediate-stage hepatocellular carcinoma.BMC Gastroenterol. 2020 Jun 29;20(1):205. doi: 10.1186/s12876-020-01355-3. BMC Gastroenterol. 2020. PMID: 32600349 Free PMC article.
-
Survival effects of postoperative adjuvant TACE in early-HCC patients with microvascular invasion: A multicenter propensity score matching.J Cancer. 2024 Jan 1;15(1):68-78. doi: 10.7150/jca.87435. eCollection 2024. J Cancer. 2024. PMID: 38164269 Free PMC article. Review.
-
Applications of propensity score matching: a case series of articles published in Annals of Coloproctology.Ann Coloproctol. 2022 Dec;38(6):398-402. doi: 10.3393/ac.2022.01060.0151. Epub 2022 Dec 28. Ann Coloproctol. 2022. PMID: 36596300 Free PMC article. Review.
Cited by
-
Transarterial chemoembolization combined with camrelizumab for recurrent hepatocellular carcinoma.BMC Cancer. 2022 Mar 14;22(1):270. doi: 10.1186/s12885-022-09325-6. BMC Cancer. 2022. PMID: 35287627 Free PMC article.
-
Which is the best TACE agent for patients with different NLR hepatocellular carcinomas? A systematic review and network meta-analysis.Heliyon. 2024 May 4;10(9):e30759. doi: 10.1016/j.heliyon.2024.e30759. eCollection 2024 May 15. Heliyon. 2024. PMID: 38765170 Free PMC article.
-
Advances and Emerging Techniques in Y-90 Radioembolization for Hepatocellular Carcinoma.Cancers (Basel). 2025 Apr 29;17(9):1494. doi: 10.3390/cancers17091494. Cancers (Basel). 2025. PMID: 40361421 Free PMC article. Review.
-
Recombinant human adenovirus p53 combined with transcatheter arterial chemoembolization for liver cancer: A meta-analysis.PLoS One. 2023 Dec 21;18(12):e0295323. doi: 10.1371/journal.pone.0295323. eCollection 2023. PLoS One. 2023. PMID: 38127912 Free PMC article.
-
Transarterial Chemoembolization Treatment Paradigms for Hepatocellular Carcinoma.Cancers (Basel). 2024 Jul 1;16(13):2430. doi: 10.3390/cancers16132430. Cancers (Basel). 2024. PMID: 39001491 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources
Miscellaneous