

Physiologically Based Pharmacokinetic Modeling of Meropenem in Preterm and Term Infants
- PMID: 34155614
- PMCID: PMC8616812
- DOI: 10.1007/s40262-021-01046-6
Physiologically Based Pharmacokinetic Modeling of Meropenem in Preterm and Term Infants
Abstract
Background: Meropenem is a broad-spectrum carbapenem antibiotic approved by the US Food and Drug Administration for use in pediatric patients, including treating complicated intra-abdominal infections in infants < 3 months of age. The impact of maturation in glomerular filtration rate and tubular secretion by renal transporters on meropenem pharmacokinetics, and the effect on meropenem dosing, remains unknown. We applied physiologically based pharmacokinetic (PBPK) modeling to characterize the disposition of meropenem in preterm and term infants.
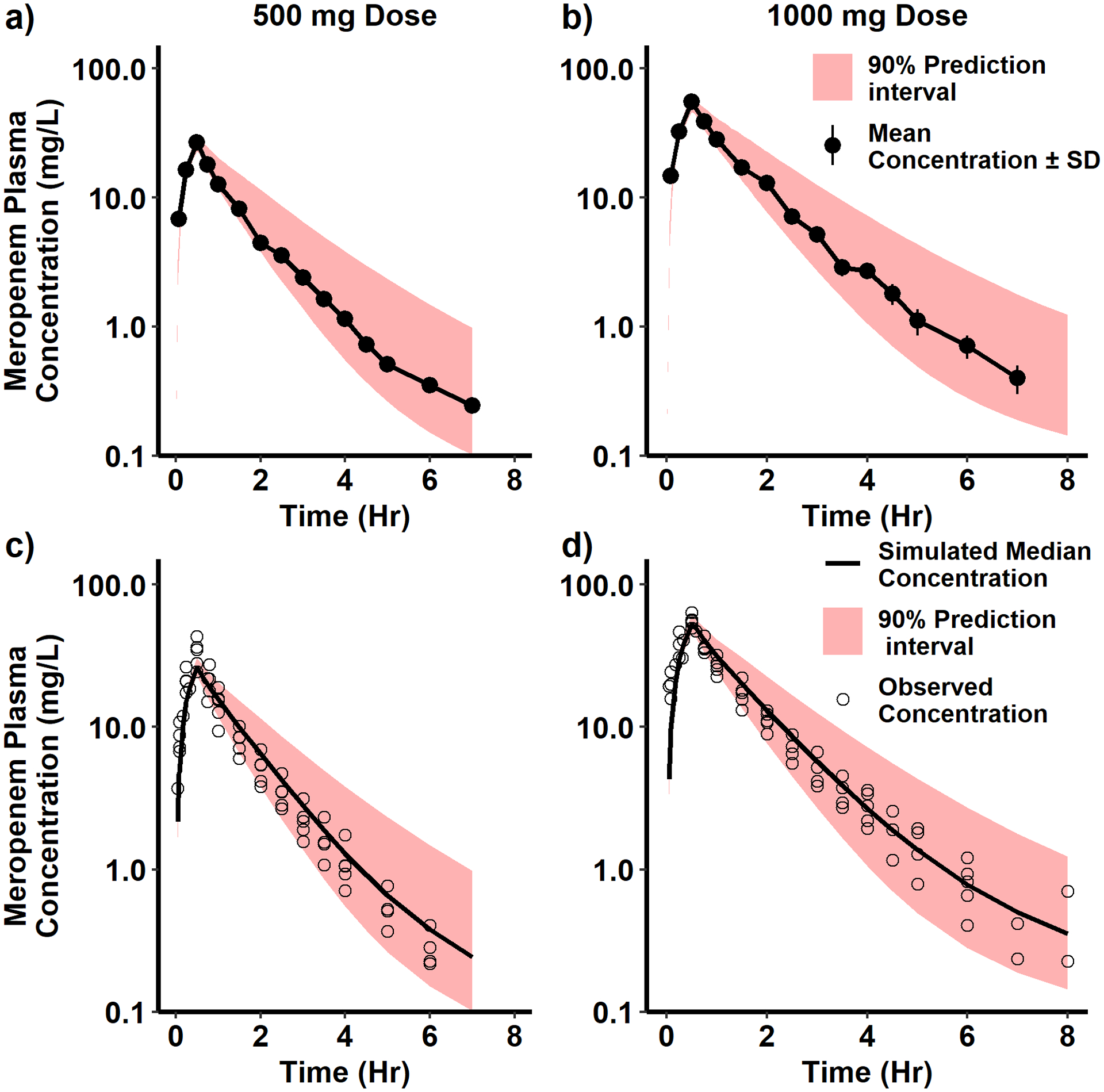
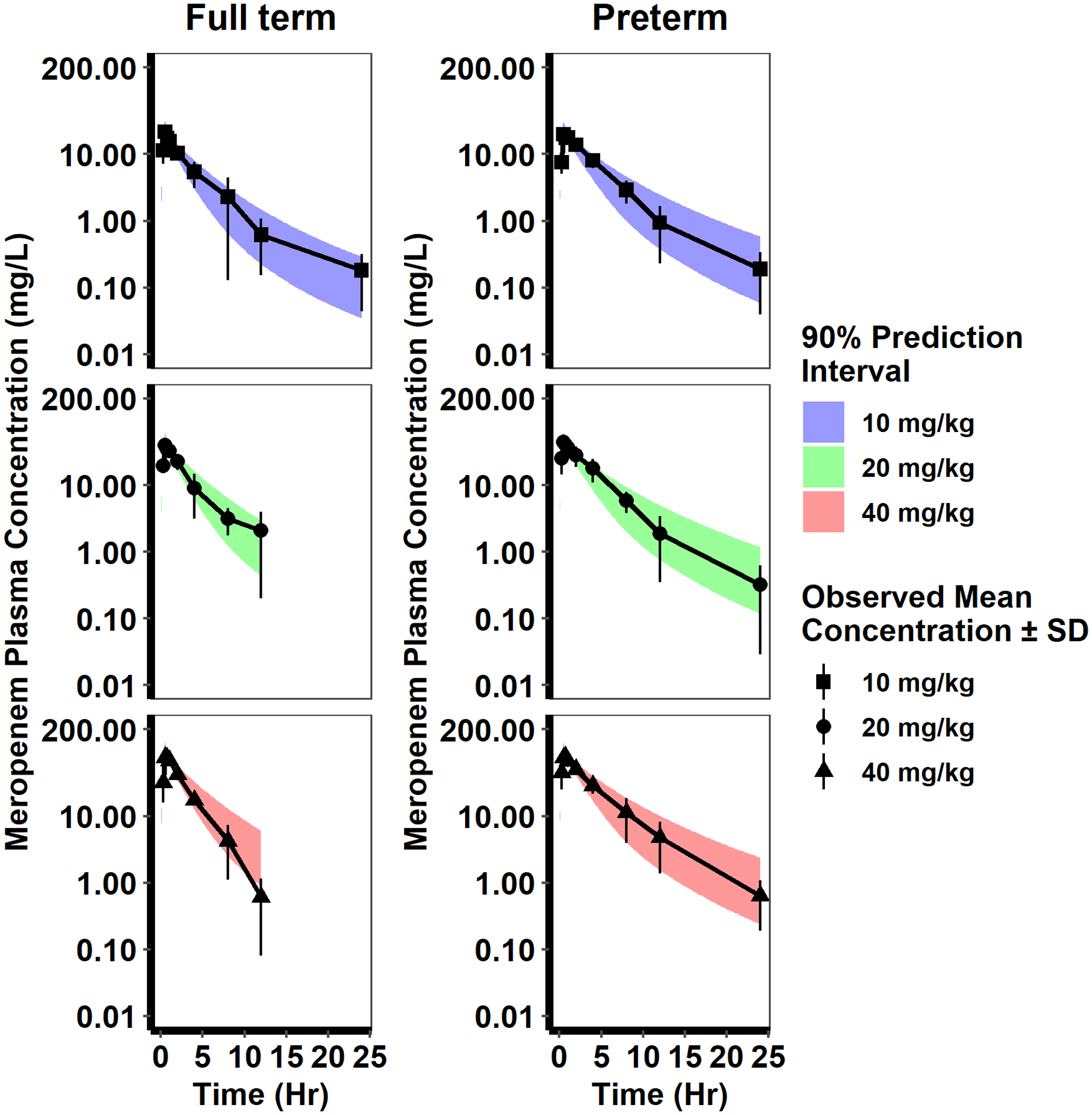
Methods: An adult meropenem PBPK model was developed in PK-Sim® (Version 8) and scaled to infants accounting for renal transporter ontogeny and glomerular filtration rate maturation. The PBPK model was evaluated using 645 plasma concentrations from 181 infants (gestational age 23-40 weeks; postnatal age 1-95 days). The PBPK model-based simulations were performed to evaluate meropenem dosing in the product label for infants < 3 months of age treated for complicated intra-abdominal infections.
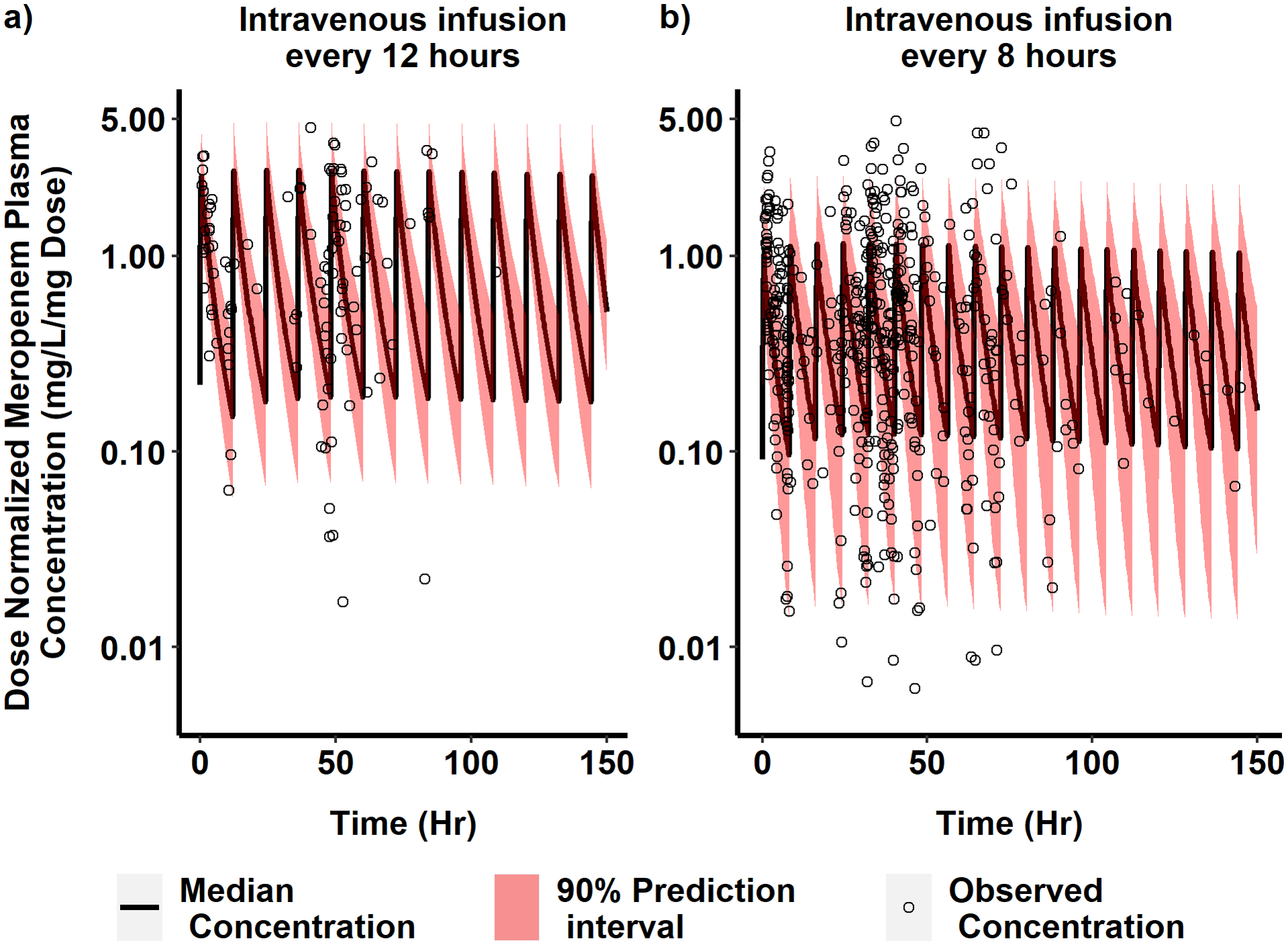
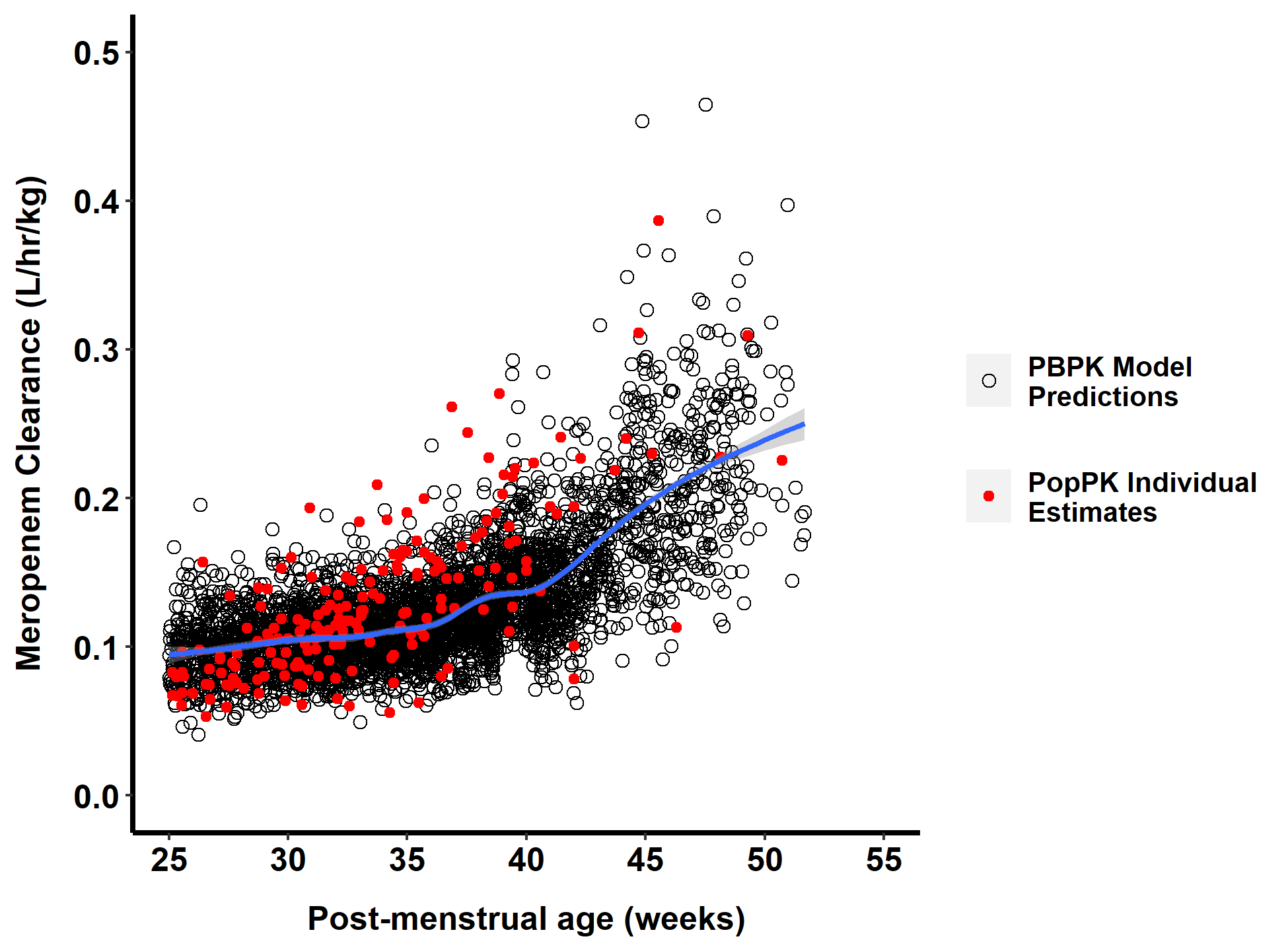
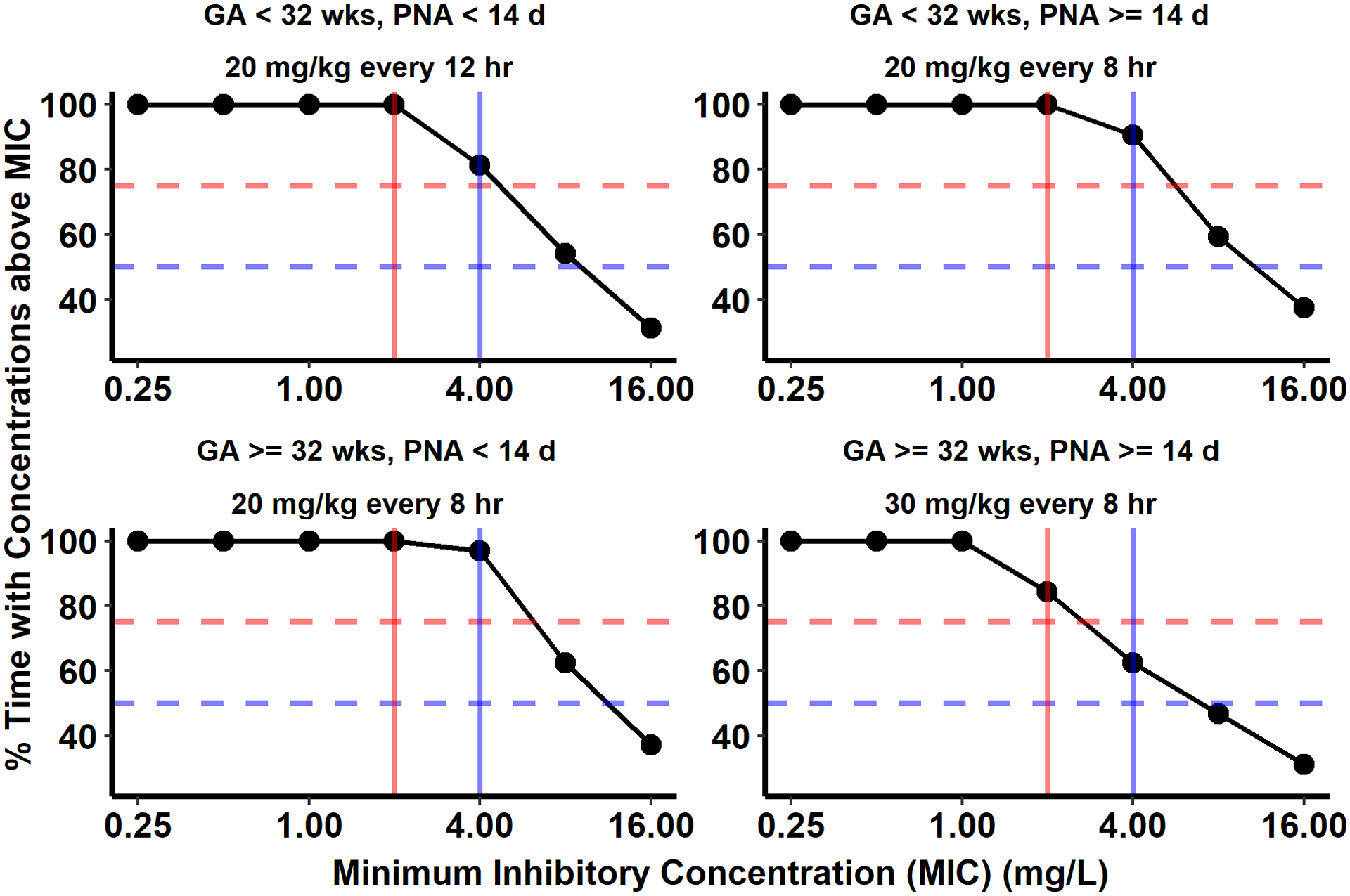
Results: Our model predicted plasma concentrations in infants in agreement with the observed data (average fold error of 0.90). The PBPK model-predicted clearance in a virtual infant population was successfully able to capture the post hoc estimated clearance of meropenem in this population, estimated by a previously published model. For 90% of virtual infants, a 4-mg/L target plasma concentration was achieved for > 50% of the dosing interval following product label-recommended dosing.
Conclusions: Our PBPK model supports the meropenem dosing regimens recommended in the product label for infants <3 months of age.
© 2021. The Author(s), under exclusive licence to Springer Nature Switzerland AG.
Figures
References
-
- MERREM(R) IV (meropenem for injection), for intravenous use <https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/050706s041lbl.pdf>(2019). Accessed May 8, 2020.
-
- Nicolau DP. Pharmacokinetic and pharmacodynamic properties of meropenem. Clin Infect Dis. 2008;47 Suppl 1:S32–40 - PubMed
-
- Turnidge JD. The pharmacodynamics of β-Lactams. Clin Infect Dis. 1998;27:10–22. - PubMed
-
- Thyrum PT, Yeh C, Birmingham B, Lasseter K. Pharmacokinetics of meropenem in patients with liver disease. Clin Infect Dis. 1997;24 Suppl 2:S184–90. - PubMed
-
- Burman LÅ, Nilsson-ehle I, Hutchison M, Haworth SJ, Norrby SR. Pharmacokinetics of meropenem and its metabolite ICI 213,689 in healthy subjects with known renal metabolism of imipenem. J Antimicrob Chemother. 1991;27:219–24. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R01 HD096435/HD/NICHD NIH HHS/United States
- K24 AI143971/AI/NIAID NIH HHS/United States
- T32 GM122741/GM/NIGMS NIH HHS/United States
- HHSN275201000003I/HD/NICHD NIH HHS/United States
- HHSN275201000003C/AA/NIAAA NIH HHS/United States
- HHSN272201300017C/AI/NIAID NIH HHS/United States
- HHSN272201300017I/AI/NIAID NIH HHS/United States
- U24 MD016258/MD/NIMHD NIH HHS/United States
- K23 HD083465/HD/NICHD NIH HHS/United States
- HHSN275201700002C/HD/NICHD NIH HHS/United States
- HHSN272201500006C/AI/NIAID NIH HHS/United States
- U18 FD006298/FD/FDA HHS/United States
LinkOut - more resources
Full Text Sources
Medical
