

Association of Intellectual Disability With All-Cause and Cause-Specific Mortality in Sweden
- PMID: 34156453
- PMCID: PMC8220491
- DOI: 10.1001/jamanetworkopen.2021.13014
Association of Intellectual Disability With All-Cause and Cause-Specific Mortality in Sweden
Abstract
Importance: Knowledge of the health challenges and mortality in people with intellectual disability (ID) should guide health policies and practices in contemporary society.
Objective: To examine premature mortality in individuals with ID.
Design, setting, and participants: This population-based longitudinal cohort study obtained data from several national health care, education, and population registers in Sweden. Two registers were used to identify individuals with ID: the National Patient Register and the Halmstad University Register on Pupils With Intellectual Disability. Two cohorts were created: cohort 1 comprised young adults (born between 1980 and 1991) with mild ID, and cohort 2 comprised individuals (born between 1932 and 2013) with mild ID or moderate to profound ID; each cohort had matched reference cohorts. Data analyses were conducted between June 1, 2020, and March 31, 2021.
Exposures: Mild or moderate to profound ID.
Main outcomes and measures: The primary outcome was overall (all-cause) mortality, and the secondary outcomes were cause-specific mortality and potentially avoidable mortality.
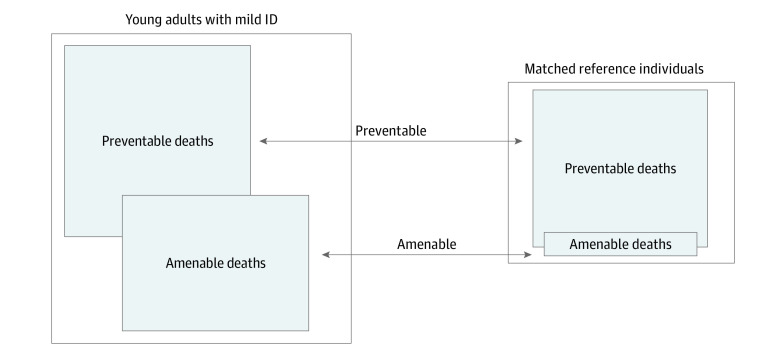
Results: Cohort 1 included 13 541 young adults with mild ID (mean [SD] age at death, 24.53 [3.66] years; 7826 men [57.8%]), and its matched reference cohort consisted of 135 410 individuals. Cohort 2 included 24 059 individuals with mild ID (mean [SD] age at death, 52.01 [16.88] years; 13 649 male individuals [56.7%]) and 26 602 individuals with moderate to profound ID (mean [SD] age at death, 42.16 [21.68] years; 15 338 male individuals [57.7%]); its matched reference cohorts consisted of 240 590 individuals with mild ID and 266 020 with moderate to profound ID. Young adults with mild ID had increased overall mortality risk compared with the matched reference cohort (odds ratio [OR], 2.86; 95% CI, 2.33-3.50), specifically excess mortality in neoplasms (OR, 3.58; 95% CI, 2.02-6.35), diseases of the nervous system (OR, 40.00; 95% CI, 18.43-86.80) and circulatory system (OR, 9.24; 95% CI, 4.76-17.95). Among deaths that were amenable to health care (OR, 7.75; 95% CI, 4.85-12.39), 55% were attributed to epilepsy. In cohort 2, increased risk of overall mortality was observed among both individuals with mild ID (OR, 6.21; 95% CI, 5.79-6.66) and moderate to profound ID (OR, 13.15; 95% CI, 12.52-13.81) compared with the matched reference cohorts. Those with moderate to profound ID had a higher risk in several cause-of-death categories compared with those with mild ID or the matched reference cohort. Adjustment for epilepsy and congenital malformations attenuated the associations. The relative risk of premature death was higher in women (OR, 6.23; 95% CI, 4.42-8.79) than in men (OR, 1.99; 95% CI, 1.53-2.60), but the absolute risk of mortality was similar (0.9% for women vs 0.9% for men).
Conclusions and relevance: This study found excess premature mortality and high risk of deaths with causes that were potentially amenable to health care intervention among people with ID. This finding suggests that this patient population faces persistent health challenges and inequality in health care encounters.
Conflict of interest statement
Figures
Comment in
-
Addressing the High Rates of Mortality in People With Intellectual Disability.JAMA Netw Open. 2021 Jun 1;4(6):e2113446. doi: 10.1001/jamanetworkopen.2021.13446. JAMA Netw Open. 2021. PMID: 34156457 No abstract available.
References
-
- American Psychiatric Association . Diagnostic and Statistical Manual of Mental Disorders. 5th ed. American Psychiatric Association; 2013.
-
- Haveman M, Heller T, Lee L, Maaskant M, Shooshtari S, Strydom A. Major health risks in aging persons with intellectual disabilities: an overview of recent studies. J Pol Pract Intellect Disabil. 2010;7(1):59-69. doi:10.1111/j.1741-1130.2010.00248.x - DOI
