

Long-term reverse remodeling and clinical improvement by MultiPoint Pacing in a randomized, international, Middle Eastern heart failure study
- PMID: 34156610
- PMCID: PMC8983631
- DOI: 10.1007/s10840-020-00928-2
Long-term reverse remodeling and clinical improvement by MultiPoint Pacing in a randomized, international, Middle Eastern heart failure study
Abstract
Purpose: Cardiac resynchronization therapy (CRT) with multipoint left ventricular (LV) pacing (MultiPoint™ Pacing, MPP) has been shown to improve CRT response, although MPP response using automated pacing vector programming has not been demonstrated in the Middle East. The purpose of this study was to compare the impact of MPP to conventional biventricular pacing (BiV) using echocardiographic and clinical changes at 6-month post-implant.
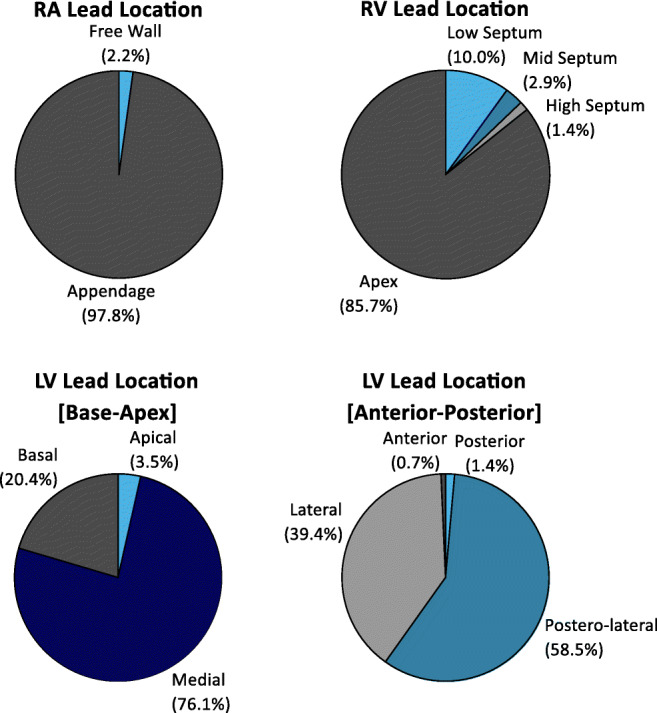
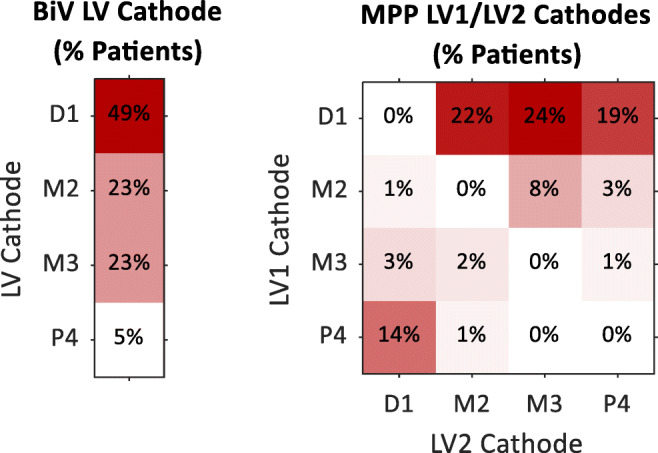
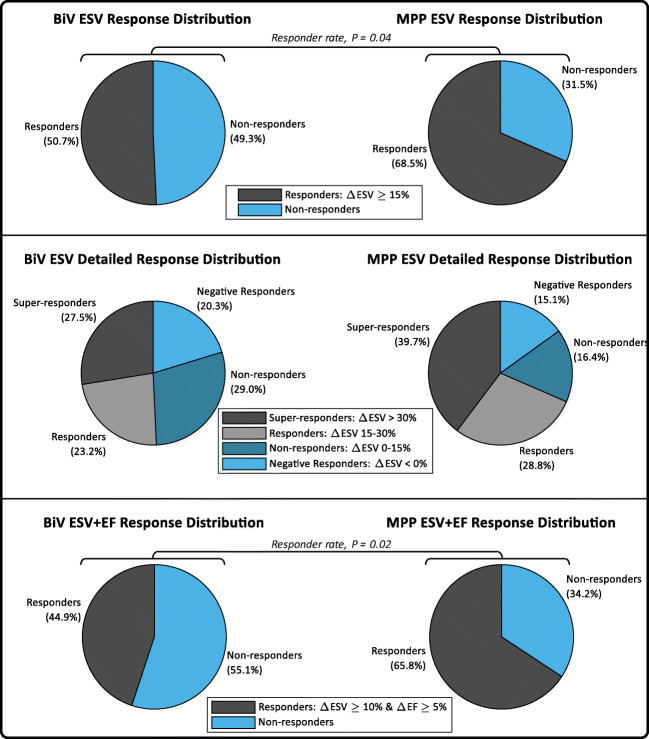
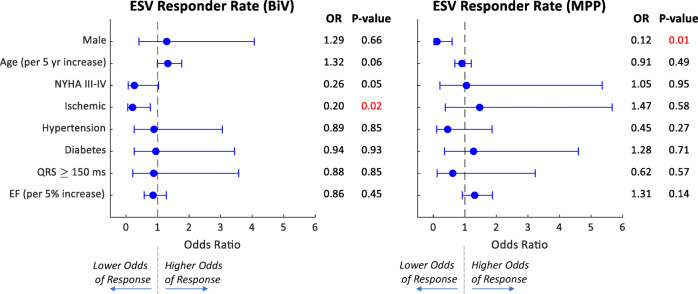
Methods: This prospective, randomized study was conducted at 13 Middle Eastern centers. After de novo CRT-D implant (Abbott Unify Quadra MP™ or Quadra Assura MP™) with quadripolar LV lead (Abbott Quartet™), patients were randomized to either BiV or MPP therapy. In BiV patients, the LV pacing vector was selected per standard practice; in MPP patients, the two LV pacing vectors were selected automatically using VectSelect. CRT response was defined at 6-month post-implant by a reduction in LV end-systolic volume (ESV) ≥ 15%.
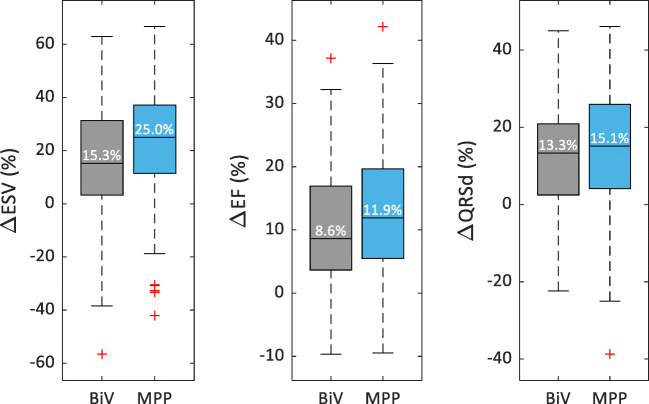
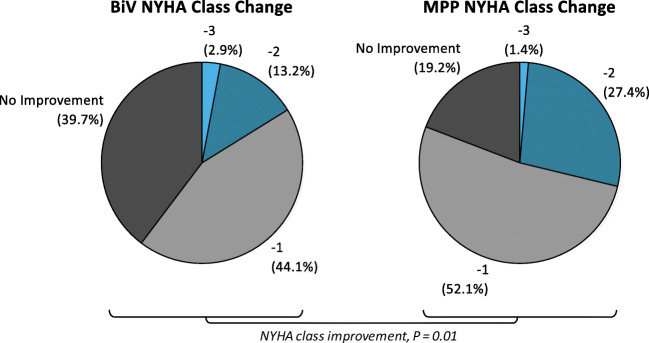
Results: One hundred and forty-two patients (61 years old, 68% male, NYHA class II/III/IV 19%/75%/6%, 33% ischemic, 57% hypertension, 52% diabetes, 158 ms QRS, 25.8% ejection fraction [EF]) were randomized to either BiV (N = 69) or MPP (N = 73). After 6 months, MPP vs. BiV patients experienced greater ESV reduction (25.0% vs. 15.3%, P = 0.08), greater EF improvement (11.9% vs. 8.6%, P = 0.36), significantly greater ESV response rate (68.5% vs. 50.7%, P = 0.04), and significantly greater NYHA class improvement rate (80.8% vs. 60.3%, P = 0.01).
Conclusions: With MPP and automatic LV vector selection, more CRT patients in the Middle East experienced reverse remodeling and clinical improvement relative to conventional BiV pacing.
Keywords: Cardiac resynchronization therapy; Heart failure; MultiPoint Pacing; Reverse remodeling.
© 2021. The Author(s).
Conflict of interest statement
Najib Al Rawahi, Fayez Bokhari, Raed Sweidan, Ahmed Al Fagih, Yahya Al Hebaishi, Ahmed Al Fagih, Ahmad Hersi, Naeem Al Shoaibi, and Maria Loricchio received research grants and/or consultancy fees from Abbott. Alexandre Chami and Nima Badie are employees of Abbott.
Figures
References
-
- Fornwalt BK, Sprague WW, BeDell P, Suever JD, Gerritse B, Merlino JD, Fyfe DA, León AR, Oshinski JN. Agreement is poor among current criteria used to define response to cardiac resynchronization therapy. Circulation. 2010;121(18):1985–1991. doi: 10.1161/CIRCULATIONAHA.109.910778. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
