

Identifying complications and failure modes of innovative growing rod configurations using the (hybrid) magnetically controlled growing rod (MCGR) and the spring distraction system (SDS)
- PMID: 34156666
- PMCID: PMC8521516
- DOI: 10.1007/s43390-021-00378-4
Identifying complications and failure modes of innovative growing rod configurations using the (hybrid) magnetically controlled growing rod (MCGR) and the spring distraction system (SDS)
Abstract
Background: Magnetically controlled growing rods (MCGRs) offer non-invasive distractions in Early-Onset Scoliosis (EOS). However, implant-related complications are common, reducing its cost-effectiveness. To improve MCGRs functionality and cost-effectiveness, we often combine a single MCGR with a contralateral sliding rod (hybrid MCGR). Recently, we developed the spring distraction system (SDS) as an alternative, which provides continuous distraction forces through a helical spring. This study aims to identify complication rates and failure modes of EOS patients treated with either of these innovative systems.
Methods: This single-centre retrospective study included EOS patients treated with a (hybrid) MCGR or SDS between 2013 and 2018. Baseline demographics, and data regarding complications and implant growth were measured. Complication rate, complication profile, complication-free survival and implant growth were compared between groups.
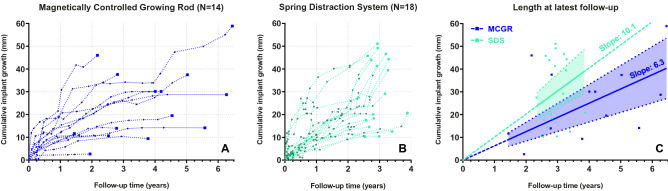
Results: Eleven hybrid- and three bilateral MCGR patients (4.1-year follow-up) and one unilateral, eleven hybrid and six bilateral SDS patients (3.0-year follow-up) were included. Groups had similar age, sex, aetiology distribution, and pre-operative Cobb angle. Complication rate was 0.35 complications/patient/year for MCGR patients and 0.33 complications/patient/year for SDS patients. The most common complications were failure to distract (MCGR-group; 8/20 complications) and implant prominence (SDS-group; 5/18 complications). Median complication-free survival was 2.6 years, with no differences between groups (p = 0.673). Implant growth was significantly higher in the SDS-group (10.1 mm/year), compared to the MCGR-group (6.3 mm/year).
Conclusion: (Hybrid) MCGR and SDS patients have similar complication rates and complication-free survival. Complication profile differs between the groups, with frequent failure to distract leading to significantly reduced implant growth in (hybrid) MCGR patients, whereas SDS patients frequently exhibit implant prominence and implant kyphosis.
Level of evidence: III.
Keywords: Complications; Early-onset scoliosis; Growth-friendly; Implant failure; Magnetically controlled growing rod; Spring distraction system.
© 2021. The Author(s).
Conflict of interest statement
J.V.C. Lemans and C.S. Tabeling report no conflicts of interest. R.M. Castelein and M.C. Kruyt report a Stryker Spine Research Grant unrelated to the current research. R.M. Castelein and M.C. Kruyt are the inventors of the spring distraction system (patent owned by UMC Utrecht Holding B.V.).
Figures





References
-
- U.S. Food and Drug Administration. FDA review results in new warnings about using general anesthetics and sedation drug in young children and pregnant women. 2016
-
- Beaven A, Gardner AC, Marks DS, Mehta JS, Newton-Ede M, Spilsbury JB. Magnetically controlled growing rods: The experience of mechanical failure from a single center consecutive series of 28 children with a minimum follow-up of 2 years. Asian Spine J. 2018;12:794–802. doi: 10.31616/ASJ.2018.12.5.794. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials