

Neonates With Tracheomalacia Generate Auto-Positive End-Expiratory Pressure via Glottis Closure
- PMID: 34157310
- PMCID: PMC8692107
- DOI: 10.1016/j.chest.2021.06.021
Neonates With Tracheomalacia Generate Auto-Positive End-Expiratory Pressure via Glottis Closure
Abstract
Background: In pediatrics, tracheomalacia is an airway condition that causes tracheal lumen collapse during breathing and may lead to the patient requiring respiratory support. Adult patients can narrow their glottis to self-generate positive end-expiratory pressure (PEEP) to raise the pressure in the trachea and prevent collapse. However, auto-PEEP has not been studied in newborns with tracheomalacia. The objective of this study was to measure the glottis cross-sectional area throughout the breathing cycle and to quantify total pressure difference through the glottis in patients with and without tracheomalacia.
Research question: Do neonates with tracheomalacia narrow their glottises? How does the glottis narrowing affect the total pressure along the airway?
Study design and methods: Ultrashort echo time MRI was performed in 21 neonatal ICU patients (11 with tracheomalacia, 10 without tracheomalacia). MRI scans were reconstructed at four different phases of breathing. All patients were breathing room air or using noninvasive respiratory support at the time of MRI. Computational fluid dynamics simulations were performed on patient-specific virtual airway models with airway anatomic features and motion derived via MRI to quantify the total pressure difference through the glottis and trachea.
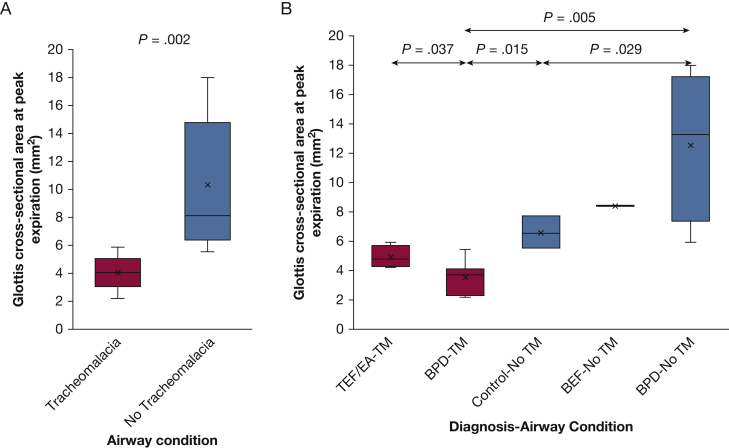
Results: The mean glottis cross-sectional area at peak expiration in the patients with tracheomalacia was less than half that in patients without tracheomalacia (4.0 ± 1.1 mm2 vs 10.3 ± 4.4 mm2; P = .002). The mean total pressure difference through the glottis at peak expiration was more than 10 times higher in patients with tracheomalacia compared with patients without tracheomalacia (2.88 ± 2.29 cm H2O vs 0.26 ± 0.16 cm H2O; P = .005).
Interpretation: Neonates with tracheomalacia narrow their glottises, which raises pressure in the trachea during expiration, thereby acting as auto-PEEP.
Keywords: BPD; auto-PEEP; computational fluid dynamics; glottis; tracheomalacia.
Copyright © 2021 American College of Chest Physicians. Published by Elsevier Inc. All rights reserved.
Figures





References
-
- McCubbin M., Frey E.E., Wagener J.S., Tribby R., Smith W.L. Large airway collapse in bronchopulmonary dysplasia. J Pediatr. 1989;114:304–307. - PubMed
-
- Boogaard R., Huijsmans S.H., Pijnenburg M.W.H., Tiddens H.A.W.M., De Jongste J.C., Merkus P.J.F.M. Tracheomalacia and bronchomalacia in children: Incidence and patient characteristics. Chest. 2005;128:3391–3397. - PubMed
-
- Carden K.A., Boiselle P.M., Waltz D.A., Ernst A. Tracheomalacia and tracheobronchomalacia in children and adults: an in-depth review. Chest. 2005;127:984–1005. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
