

Growth Rates of Infants Randomized to Continuous Positive Airway Pressure or Intubation After Extremely Preterm Birth
- PMID: 34157349
- PMCID: PMC8478787
- DOI: 10.1016/j.jpeds.2021.06.026
Growth Rates of Infants Randomized to Continuous Positive Airway Pressure or Intubation After Extremely Preterm Birth
Abstract
Objective: To evaluate the effects of early treatment with continuous positive airway pressure (CPAP) on nutritional intake and in-hospital growth rates of extremely preterm (EPT) infants.
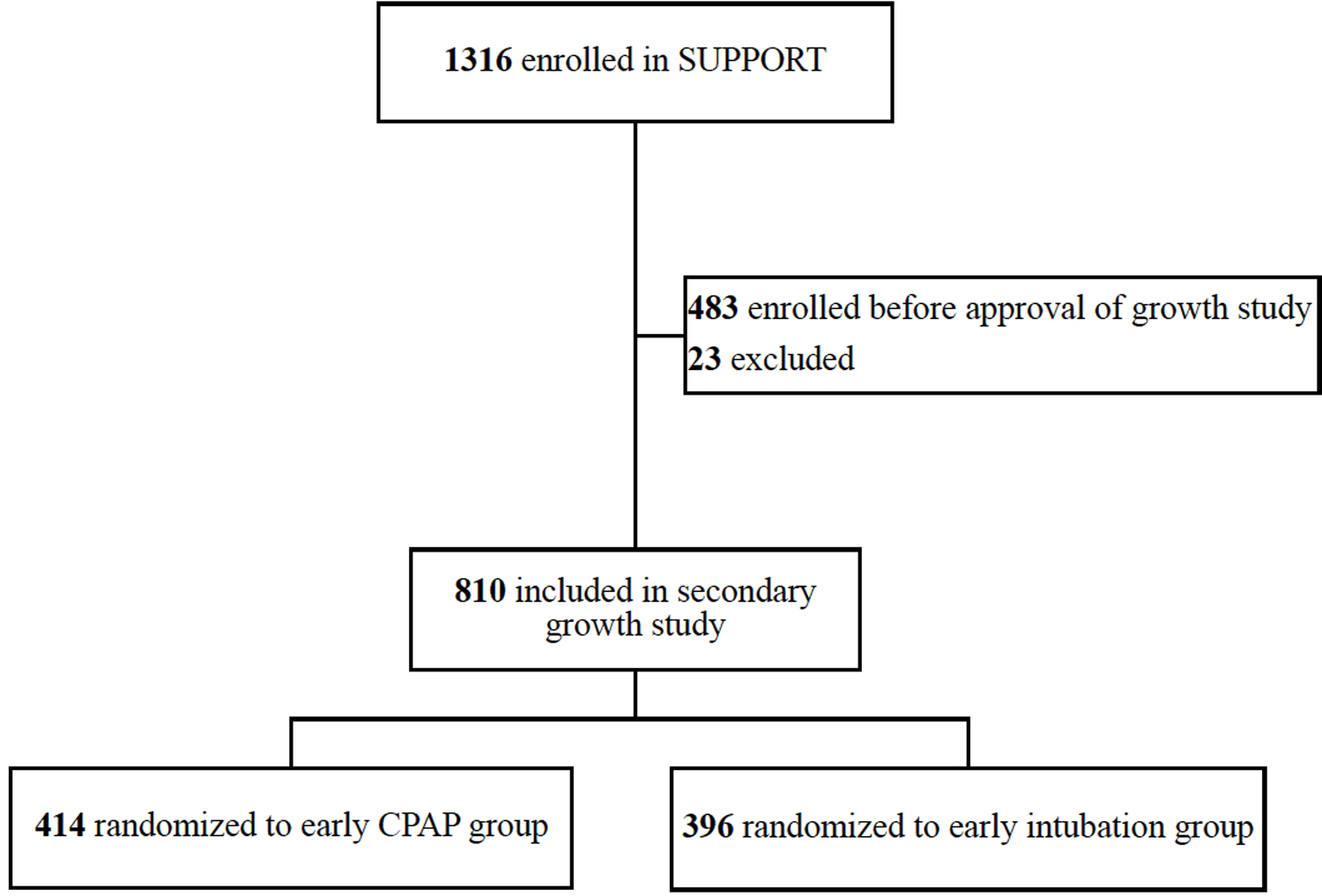
Study design: EPT infants (240/7-276/7 weeks of gestation) enrolled in the Surfactant Positive Airway Pressure and Pulse Oximetry Trial (SUPPORT) were included. EPT infants who died before 36 weeks of postmenstrual age (PMA) were excluded. The growth rates from birth to 36 weeks of PMA and follow-up outcomes at 18-22 months corrected age of EPT infants randomized at birth to either early CPAP (intervention group) or early intubation for surfactant administration (control group) were analyzed.
Results: Growth data were analyzed for 810 of 1316 infants enrolled in SUPPORT (414 in the intervention group, 396 in the control group). The median gestational age was 26 weeks, and the mean birth weight was 839 g. Baseline characteristics, total nutritional intake, and in-hospital comorbidities were not significantly different between the 2 groups. In a regression model, growth rates between birth and 36 weeks of PMA, as well as growth rates during multiple intervals from birth to day 7, days 7-14, days 14-21, days 21-28, day 28 to 32 weeks PMA, and 32-36 weeks PMA did not differ between treatment groups. Independent of treatment group, higher growth rates from day 21 to day 28 were associated with a lower risk of having a Bayley-III cognitive score <85 at 18-22 months corrected age (P = .002).
Conclusions: EPT infants randomized to early CPAP did not have higher in-hospital growth rates than infants randomized to early intubation.
Copyright © 2021 Elsevier Inc. All rights reserved.
Conflict of interest statement
The other authors declare no conflicts of interest.
References
-
- Embleton ND, Morgan C, King C. Balancing the risks and benefits of parenteral nutrition for preterm infants: can we define the optimal composition? Arch Dis Child Fetal Neonatal Ed. 2015;100:F72–5. - PubMed
-
- Embleton NE, Pang N, Cooke RJ. Postnatal malnutrition and growth retardation: an inevitable consequence of current recommendations in preterm infants? Pediatrics. 2001;107:270–3. - PubMed
-
- Fenton TR, Anderson D, Groh-Wargo S, Hoyos A, Ehrenkranz RA, Senterre T. An Attempt to Standardize the Calculation of Growth Velocity of Preterm Infants-Evaluation of Practical Bedside Methods. J Pediatr. 2018;196:77–83. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- UG1 HD068263/HD/NICHD NIH HHS/United States
- U10 HD021373/HD/NICHD NIH HHS/United States
- K23 HD102554/HD/NICHD NIH HHS/United States
- UG1 HD087226/HD/NICHD NIH HHS/United States
- U01 HD036790/HD/NICHD NIH HHS/United States
- K23 DK120960/DK/NIDDK NIH HHS/United States
- UG1 HD068270/HD/NICHD NIH HHS/United States
- UG1 HD053089/HD/NICHD NIH HHS/United States
- UG1 HD027856/HD/NICHD NIH HHS/United States
- UG1 HD034216/HD/NICHD NIH HHS/United States
- UG1 HD027904/HD/NICHD NIH HHS/United States
- UG1 HD027880/HD/NICHD NIH HHS/United States
- U10 HD068284/HD/NICHD NIH HHS/United States
- UG1 HD053109/HD/NICHD NIH HHS/United States
- UG1 HD027851/HD/NICHD NIH HHS/United States
- U10 HD036790/HD/NICHD NIH HHS/United States
- UG1 HD068244/HD/NICHD NIH HHS/United States
- UG1 HD027853/HD/NICHD NIH HHS/United States
- UG1 HD087229/HD/NICHD NIH HHS/United States
- UL1 TR003167/TR/NCATS NIH HHS/United States
- UG1 HD040689/HD/NICHD NIH HHS/United States
- UG1 HD068284/HD/NICHD NIH HHS/United States
- UG1 HD021385/HD/NICHD NIH HHS/United States
- UG1 HD040492/HD/NICHD NIH HHS/United States
- UG1 HD021364/HD/NICHD NIH HHS/United States
- UG1 HD068278/HD/NICHD NIH HHS/United States
- U24 HD095254/HD/NICHD NIH HHS/United States
