

Deep learning radiomics-based prediction of distant metastasis in patients with locally advanced rectal cancer after neoadjuvant chemoradiotherapy: A multicentre study
- PMID: 34157487
- PMCID: PMC8237293
- DOI: 10.1016/j.ebiom.2021.103442
Deep learning radiomics-based prediction of distant metastasis in patients with locally advanced rectal cancer after neoadjuvant chemoradiotherapy: A multicentre study
Abstract
Background: Accurate predictions of distant metastasis (DM) in locally advanced rectal cancer (LARC) patients receiving neoadjuvant chemoradiotherapy (nCRT) are helpful in developing appropriate treatment plans. This study aimed to perform DM prediction through deep learning radiomics.
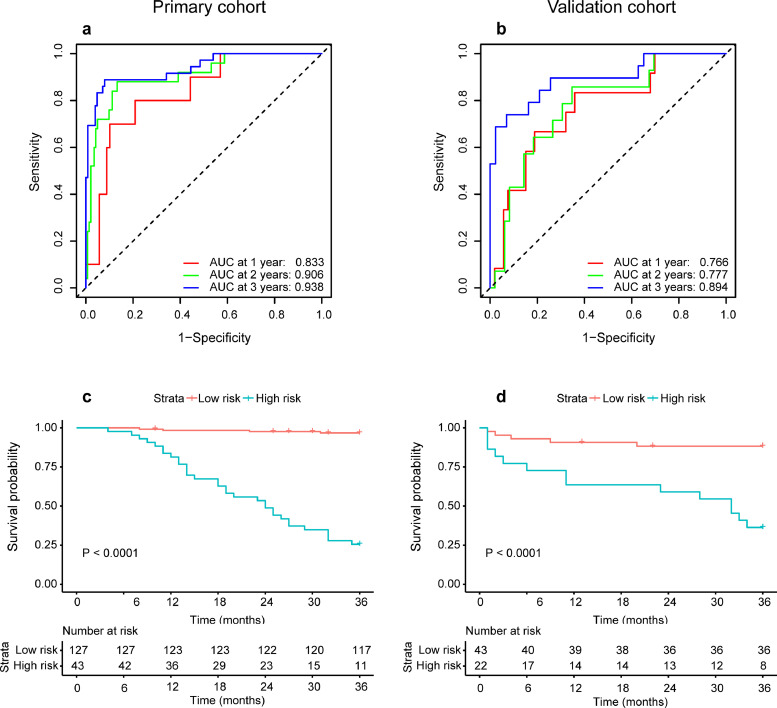
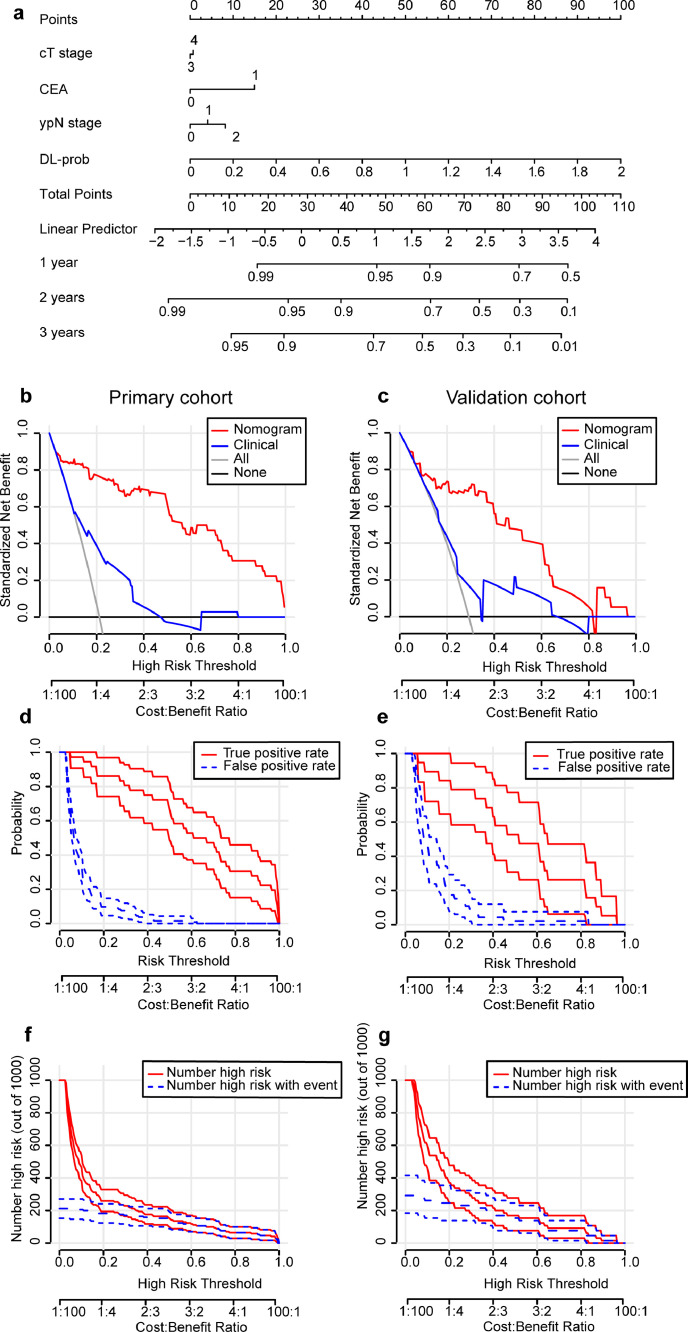
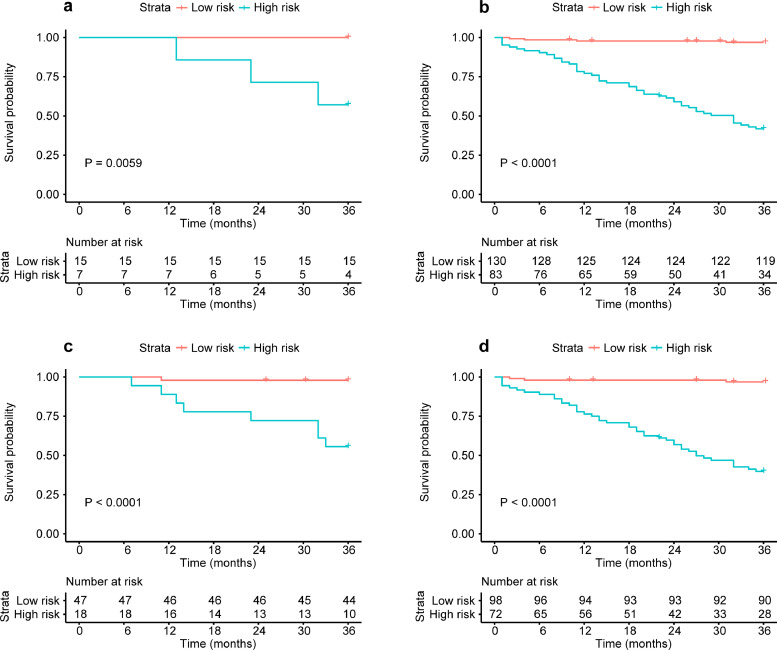
Methods: We retrospectively sampled 235 patients receiving nCRT with the minimum 36 months' postoperative follow-up from three hospitals. Through transfer learning, a deep learning radiomic signature (DLRS) based on multiparametric magnetic resonance imaging (MRI) was constructed. A nomogram was established integrating deep MRI information and clinicopathologic factors for better prediction. Harrell's concordance index (C-index) and time-dependent receiver operating characteristic (ROC) were used as performance metrics. Furthermore, the risk of DM in patients with different response to nCRT was evaluated with the nomogram.
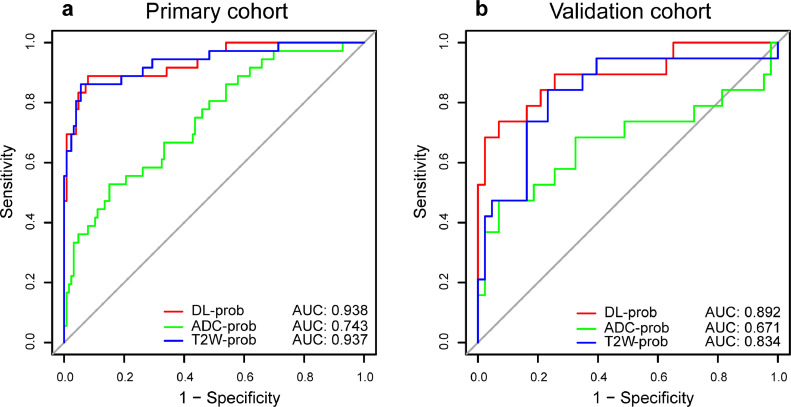
Findings: DLRS performed well in DM prediction, with a C-index of 0·747 and an area under curve (AUC) at three years of 0·894 in the validation cohort. The performance of nomogram was better, with a C-index of 0·775. In addition, the nomogram could stratify patients with different responses to nCRT into high- and low-risk groups of DM (P < 0·05).
Interpretation: MRI-based deep learning radiomics had potential in predicting the DM of LARC patients receiving nCRT and could help evaluate the risk of DM in patients who have different responses to nCRT.
Funding: The funding bodies that contributed to this study are listed in the Acknowledgements section.
Keywords: Deep learning radiomics; Distant metastasis; Locally advanced rectal cancer; Magnetic resonance imaging; Neoadjuvant chemoradiotherapy.
Copyright © 2021 The Authors. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest The authors have declared that no competing interest exists.
Figures
Similar articles
-
Predicting pathological complete response following neoadjuvant chemoradiotherapy (nCRT) in patients with locally advanced rectal cancer using merged model integrating MRI-based radiomics and deep learning data.BMC Med Imaging. 2024 Oct 24;24(1):289. doi: 10.1186/s12880-024-01474-3. BMC Med Imaging. 2024. PMID: 39448917 Free PMC article.
-
MRI-based Multiregional Radiomics for Pretreatment Prediction of Distant Metastasis After Neoadjuvant Chemoradiotherapy in Patients with Locally Advanced Rectal Cancer.Acad Radiol. 2024 Apr;31(4):1367-1377. doi: 10.1016/j.acra.2023.09.007. Epub 2023 Oct 4. Acad Radiol. 2024. PMID: 37802671
-
Radiomics signature as a new biomarker for preoperative prediction of neoadjuvant chemoradiotherapy response in locally advanced rectal cancer.Diagn Interv Radiol. 2021 May;27(3):308-314. doi: 10.5152/dir.2021.19677. Diagn Interv Radiol. 2021. PMID: 34003118 Free PMC article.
-
Machine learning in predicting pathological complete response to neoadjuvant chemoradiotherapy in rectal cancer using MRI: a systematic review and meta-analysis.Br J Radiol. 2024 Jun 18;97(1159):1243-1254. doi: 10.1093/bjr/tqae098. Br J Radiol. 2024. PMID: 38730550 Free PMC article.
-
Significance of MRI-based radiomics in predicting pathological complete response to neoadjuvant chemoradiotherapy of locally advanced rectal cancer: A narrative review.Cancer Radiother. 2024 Aug;28(4):390-401. doi: 10.1016/j.canrad.2024.04.003. Epub 2024 Aug 22. Cancer Radiother. 2024. PMID: 39174361 Review.
Cited by
-
Deep learning-based automated high-accuracy location and identification of fresh vertebral compression fractures from spinal radiographs: a multicenter cohort study.Front Bioeng Biotechnol. 2024 May 14;12:1397003. doi: 10.3389/fbioe.2024.1397003. eCollection 2024. Front Bioeng Biotechnol. 2024. PMID: 38812917 Free PMC article.
-
Three-dimensional deep learning model complements existing models for preoperative disease-free survival prediction in localized clear cell renal cell carcinoma: a multicenter retrospective cohort study.Int J Surg. 2024 Nov 1;110(11):7034-7046. doi: 10.1097/JS9.0000000000001808. Int J Surg. 2024. PMID: 38896853 Free PMC article.
-
Deep learning radiomics and mediastinal adipose tissue-based nomogram for preoperative prediction of postoperative brain metastasis risk in non-small cell lung cancer.BMC Cancer. 2025 Jul 1;25(1):1133. doi: 10.1186/s12885-025-14466-5. BMC Cancer. 2025. PMID: 40597925 Free PMC article.
-
Interpretable MRI Subregional Radiomics-Deep Learning Model for Preoperative Lymphovascular Invasion Prediction in Rectal Cancer: A Dual-Center Study.J Imaging Inform Med. 2025 Jul 11. doi: 10.1007/s10278-025-01586-4. Online ahead of print. J Imaging Inform Med. 2025. PMID: 40646374
-
Deep learning-based quantification of tumor-infiltrating lymphocytes as a prognostic indicator in nasopharyngeal carcinoma: multicohort findings.ESMO Open. 2025 Jul;10(7):105494. doi: 10.1016/j.esmoop.2025.105494. Epub 2025 Jul 3. ESMO Open. 2025. PMID: 40614660 Free PMC article.
References
-
- Sauer R, Liersch T, Merkel S. Preoperative versus postoperative chemoradiotherapy for locally advanced rectal cancer: results of the German CAO/ARO/AIO-94 randomized phase III trial after a median follow-up of 11 years. J Clin Oncol. 2012;30:1926–1933. - PubMed
-
- Peeters KCMJ, Marijnen CAM, Nagtegaal ID. The TME trial after a median follow-up of 6 years: increased local control but no survival benefit in irradiated patients with resectable rectal carcinoma. Ann Surg. 2007;246:693–701. - PubMed
-
- Glynne-Jones R, Wyrwicz L, Tiret E. Rectal cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2017;28:22–40. iv. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
