

Guideline interval: A new time interval in the diagnostic pathway for symptomatic cancer
- PMID: 34157609
- PMCID: PMC8316604
- DOI: 10.1016/j.canep.2021.101969
Guideline interval: A new time interval in the diagnostic pathway for symptomatic cancer
Abstract
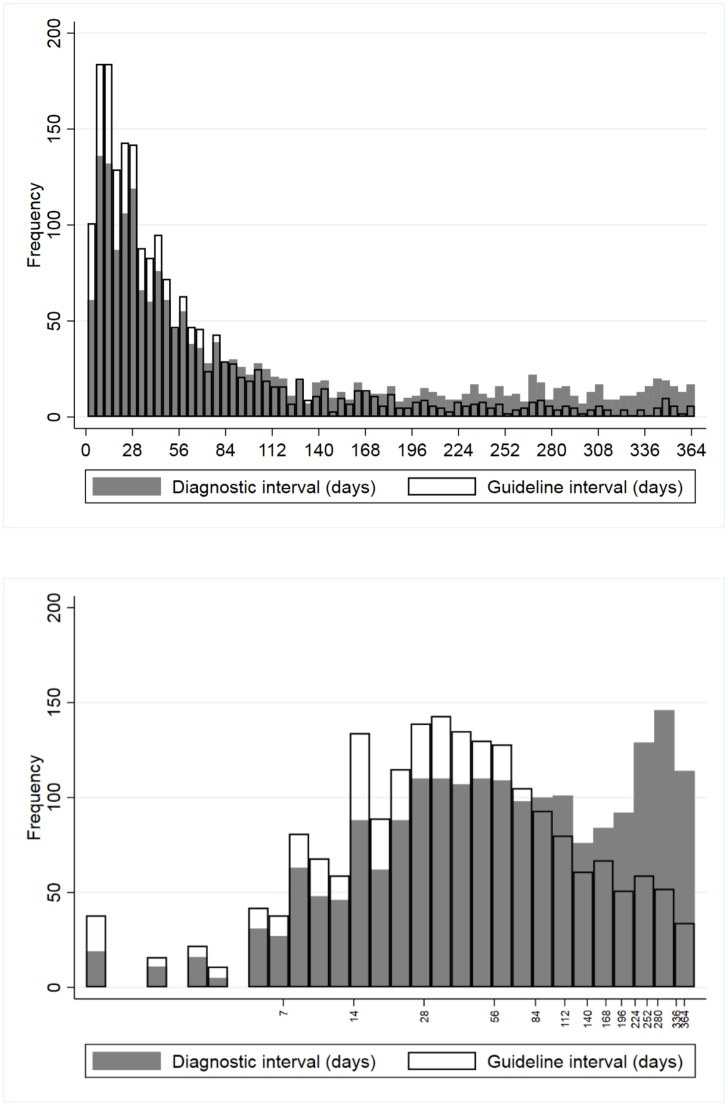
Background: A standard measure of the cancer diagnostic pathway, diagnostic interval, is the time from "first presentation of cancer" to diagnosis. Cancer presentation may be unclear in patients with multimorbidity or non-specific symptoms, signs or test results ("features"). We propose an alternative, guideline interval, with a more certain start date; namely, when the patient first meets suspected-cancer criteria for investigation or referral.
Methods: This retrospective cohort study used Clinical Practice Research Datalink (CPRD) and English cancer registry data. Participants, aged ≥55 years, had diagnostic codes for oesophagogastric cancers in 1/1/12-31/12/17. Features of oesophagogastric cancer in the year before diagnosis were identified from CPRD codes for dysphagia, haematemesis, upper-abdominal mass or pain, low haemoglobin, reflux, dyspepsia, nausea, vomiting, weight loss or thrombocytosis. Diagnostic interval was the time from first feature to diagnosis; guidance interval, the time from first meeting criteria in NICE suspected-cancer guidance to diagnosis. Multimorbidity burden was quantified using Adjusted Clinical Groups®. Accelerated failure-time models explored associations between multimorbidity burden and length of both diagnostic and guideline interval.
Results: There were 3,793 eligible participants (69.0 % male), mean age 74.1 years (SD 10.5). 3,097 (81.7 %) presented with ≥1 feature in the year before diagnosis, and 1,990 (52.5 %) met NICE suspected-cancer criteria. The median for both intervals was 11 days in healthy users, and rose with increasing morbidity burden. At very high multimorbidity burden, diagnostic interval was 5.47 (95%CI 3.25-9.20) times longer and guideline interval was 3.91 (2.63-5.80) times longer than for healthy users.
Conclusions: Guideline interval is proposed as a new measure of the cancer diagnostic pathway. It has a more certain start date than diagnostic interval, and is lengthened less than diagnostic interval in people with a very high multimorbidity burden. Guideline interval has potential for assessing the implementation of suspected-cancer policies.
Keywords: Databases and data mining; Diagnostic interval; Electronic health records; Modelling healthcare services.
Copyright © 2021. Published by Elsevier Ltd.
Conflict of interest statement
The authors report no declarations of interest.
Figures
Similar articles
-
Quantifying the impact of pre-existing conditions on the stage of oesophagogastric cancer at diagnosis: a primary care cohort study using electronic medical records.Fam Pract. 2021 Jul 28;38(4):425-431. doi: 10.1093/fampra/cmaa132. Fam Pract. 2021. PMID: 33346832 Free PMC article.
-
Age and Gender Variations in Cancer Diagnostic Intervals in 15 Cancers: Analysis of Data from the UK Clinical Practice Research Datalink.PLoS One. 2015 May 15;10(5):e0127717. doi: 10.1371/journal.pone.0127717. eCollection 2015. PLoS One. 2015. PMID: 25978414 Free PMC article.
-
Trends in time to cancer diagnosis around the period of changing national guidance on referral of symptomatic patients: A serial cross-sectional study using UK electronic healthcare records from 2006-17.Cancer Epidemiol. 2020 Dec;69:101805. doi: 10.1016/j.canep.2020.101805. Epub 2020 Sep 9. Cancer Epidemiol. 2020. PMID: 32919226 Free PMC article.
-
Understanding ethnic inequalities in cancer diagnostic intervals: a cohort study of patients presenting suspected cancer symptoms to GPs in England.Br J Gen Pract. 2025 May 2;75(754):e333-e340. doi: 10.3399/BJGP.2024.0518. Print 2025 May. Br J Gen Pract. 2025. PMID: 39689922 Free PMC article.
-
Evidence reviews for diagnostic accuracy of prostate specific antigen (PSA) thresholds for referring people with suspected prostate cancer: Suspected cancer: recognition and referral: Evidence review A.London: National Institute for Health and Care Excellence (NICE); 2021 Dec. London: National Institute for Health and Care Excellence (NICE); 2021 Dec. PMID: 37200463 Free Books & Documents. Review.
References
-
- NHS . Department of Health; London: 2019. NHS Long Term Plan.
-
- Weller D., Vedsted P., Rubin G., Walter F.M., Emery J., Scott S., Campbell C., Andersen R.S., Hamilton W., Olesen F., Rose P., Nafees S., van Rijswijk E., Hiom S., Muth C., Beyer M., Neal R.D. The Aarhus statement: improving design and reporting of studies on early cancer diagnosis. Br. J. Cancer. 2012;106(7):1262–1267. - PMC - PubMed
-
- Price S., Spencer A., Zhang X., Ball S., Lyratzopoulos G., Mujica-Mota R., Stapley S., Ukoumunne O.C., Hamilton W. Trends in time to cancer diagnosis around the period of changing national guidance on referral of symptomatic patients: a serial cross-sectional study using UK electronic healthcare records from 2006–17. Cancer Epidemiol. 2020;69 101805-101805. - PMC - PubMed
-
- Weller D., Menon U., Zalounina Falborg A., Jensen H., Barisic A., Knudsen A.K., Bergin R.J., Brewster D.H., Cairnduff V., Gavin A.T., Grunfeld E., Harland E., Lambe M., Law R.-J., Lin Y., Malmberg M., Turner D., Neal R.D., White V., Harrison S., Reguilon I., Vedsted P. Diagnostic routes and time intervals for patients with colorectal cancer in 10 international jurisdictions; findings from a cross-sectional study from the International Cancer Benchmarking Partnership (ICBP) BMJ Open. 2018;8(11) - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
