

Extravasation Injuries of the Limbs in Neonates and Children—Development of a Treatment Algorithm
- PMID: 34158148
- PMCID: PMC8579427
- DOI: 10.3238/arztebl.m2021.0220
Extravasation Injuries of the Limbs in Neonates and Children—Development of a Treatment Algorithm
Abstract
Background: Children and neonates very often receive intravenous therapy. There is a lack of systematic data on the incidence of extravasation injuries in children and neonates. Individual studies involving neonates receiving intravenous therapy on intensive care units report incidence rates of 18-46%. Serious complications, such as necrosis and ulceration, develop in 2.4-4% of cases, which in the long term can lead to contractures, deformities, and loss of limb function secondary to unfavorable scar formation. There are no guidelines available to date on the management of pediatric extravasation injuries.
Methods: The present review article is based on a selective search of the literature in PubMed (for the period 1979 until June 2020) and our own clinical experience.
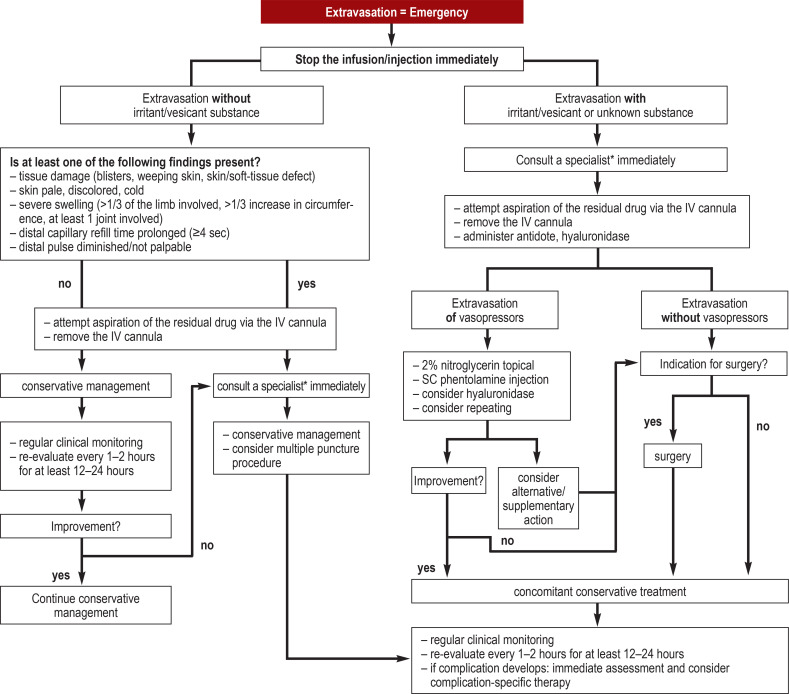
Results: There is a lack of randomized controlled studies on the management of pediatric extravasation injuries, so the level of evidence remains restricted to small comparative studies and case series. Conservative, pharmacological or surgical forms of treatment are used, depending on the volume and type of extravasated fluid as well as patient-specific factors. Firstly, an assessment is made as to whether the extravasated fluid is a substance with no primary toxic properties, a tissue irritating (irritant), or a necrosis-inducing (vesicant) substance. Skin and tissue should be examined for damage, skin color, swelling, capillary refill time, and pulse (distal to the injury). Depending on the substance and volume of the extravasated fluid and the degree of tissue damage, treatment options include conservative forms of treatment, administration of antidotes, hyaluronidase or vasodilators (such as phentolamine), the multiple puncture procedure, flushouts, and liposuction.
Conclusion: Without evidence for the superiority of any particular treatment, therapy remains an individual decision, carrying the risks associated with off-label use.
Figures

Comment in
-
An interdisciplinary approach is required.Dtsch Arztebl Int. 2022 Mar 18;119(11):199. doi: 10.3238/arztebl.m2022.0044. Dtsch Arztebl Int. 2022. PMID: 35655352 Free PMC article. No abstract available.
-
In reply.Dtsch Arztebl Int. 2022 Mar 18;119(11):199-200. doi: 10.3238/arztebl.m2022.0045. Dtsch Arztebl Int. 2022. PMID: 35655353 Free PMC article. No abstract available.
Similar articles
-
Incidence, risk factors and treatment outcomes of drug extravasation in pediatric patients in China.Turk J Pediatr. 2017;59(2):1621-168. doi: 10.24953/turkjped.2017.02.008. Turk J Pediatr. 2017. PMID: 29276869
-
Severe Extravasation Injuries in Neonates: A Report of 34 Cases.Pediatr Dermatol. 2015 Nov-Dec;32(6):830-5. doi: 10.1111/pde.12664. Epub 2015 Sep 4. Pediatr Dermatol. 2015. PMID: 26337780
-
Point-of-Care Ultrasound Use in Neonatal Peripheral Intravenous Extravasation Injuries: A Case Series.J Wound Ostomy Continence Nurs. 2018 Nov/Dec;45(6):503-509. doi: 10.1097/WON.0000000000000475. J Wound Ostomy Continence Nurs. 2018. PMID: 30395125
-
Treating extravasation injuries in infants and young children: a scoping review and survey of UK NHS practice.BMC Pediatr. 2019 Jan 7;19(1):6. doi: 10.1186/s12887-018-1387-1. BMC Pediatr. 2019. PMID: 30616600 Free PMC article.
-
Prevention and management of extravasation of cytotoxic drugs.Drug Saf. 1995 Apr;12(4):245-55. doi: 10.2165/00002018-199512040-00004. Drug Saf. 1995. PMID: 7646823 Review.
Cited by
-
Sensing Technologies for Extravasation Detection: A Review.ACS Sens. 2023 Mar 24;8(3):1017-1032. doi: 10.1021/acssensors.2c02602. Epub 2023 Mar 13. ACS Sens. 2023. PMID: 36912628 Free PMC article. Review.
-
Peripheral intravenous therapy infiltration/extravasation (PIVIE) risks and the potential for earlier notification of events using a novel sensor technology in a neonatal population.J Vasc Access. 2024 Nov;25(6):1801-1807. doi: 10.1177/11297298231185536. Epub 2023 Jul 3. J Vasc Access. 2024. PMID: 37395292 Free PMC article.
-
Distal Tibia Epiphysiodesis After Saphenous Vein Catheterization During Treatment for Prematurity.Cureus. 2022 Jan 25;14(1):e21596. doi: 10.7759/cureus.21596. eCollection 2022 Jan. Cureus. 2022. PMID: 35228954 Free PMC article.
-
Peripheral venous extravasation injury.BJA Educ. 2023 Feb;23(2):42-45. doi: 10.1016/j.bjae.2022.11.002. Epub 2022 Dec 22. BJA Educ. 2023. PMID: 36686886 Free PMC article. No abstract available.
-
An interdisciplinary approach is required.Dtsch Arztebl Int. 2022 Mar 18;119(11):199. doi: 10.3238/arztebl.m2022.0044. Dtsch Arztebl Int. 2022. PMID: 35655352 Free PMC article. No abstract available.
References
-
- Amjad I, Murphy T, Nylander-Housholder L, Ranft A. A new approach to management of intravenous infiltration in pediatric patients: pathophysiology, classification, and treatment. J Infus Nurs. 2011;34:242–249. - PubMed
-
- Ching D, Wong KY. Pediatric extravasation injury management: a survey comparing 10 hospitals. Pediatr Neonatol. 2017;58:549–551. - PubMed
-
- Kostogloudis N, Demiri E, Tsimponis A, et al. Severe extravasation injuries in neonates: a report of 34 cases. Pediatr Dermatol. 2015;32:830–835. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical