

Psoriatic disease is associated with systemic inflammation, endothelial activation, and altered haemostatic function
- PMID: 34158537
- PMCID: PMC8219816
- DOI: 10.1038/s41598-021-90684-8
Psoriatic disease is associated with systemic inflammation, endothelial activation, and altered haemostatic function
Abstract
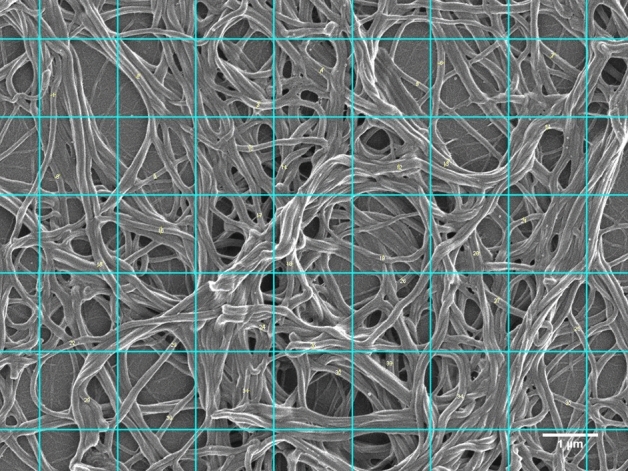
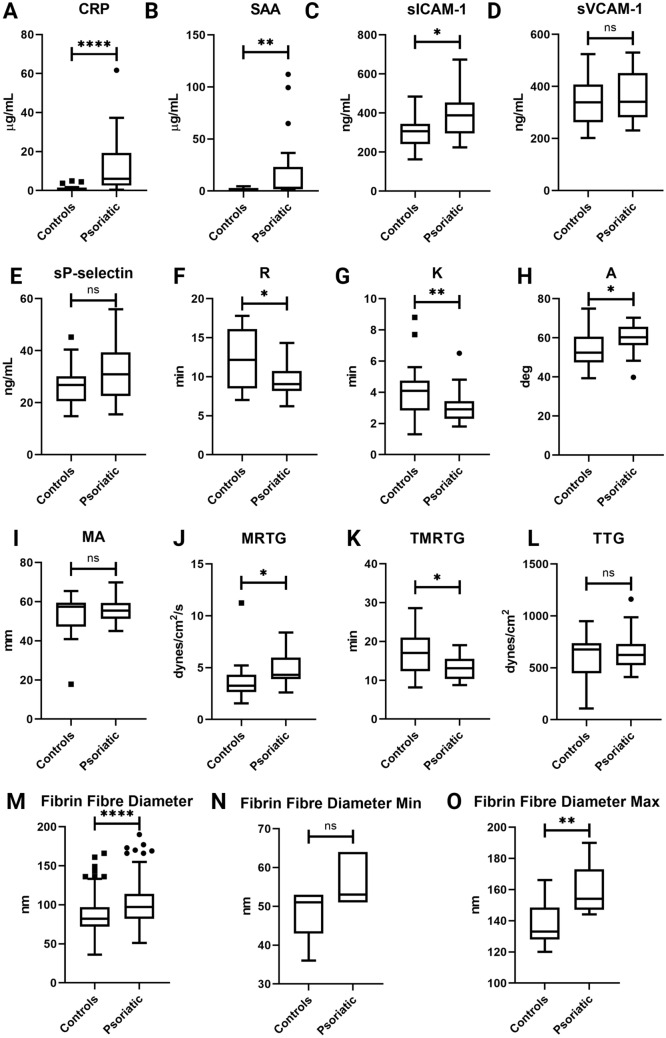
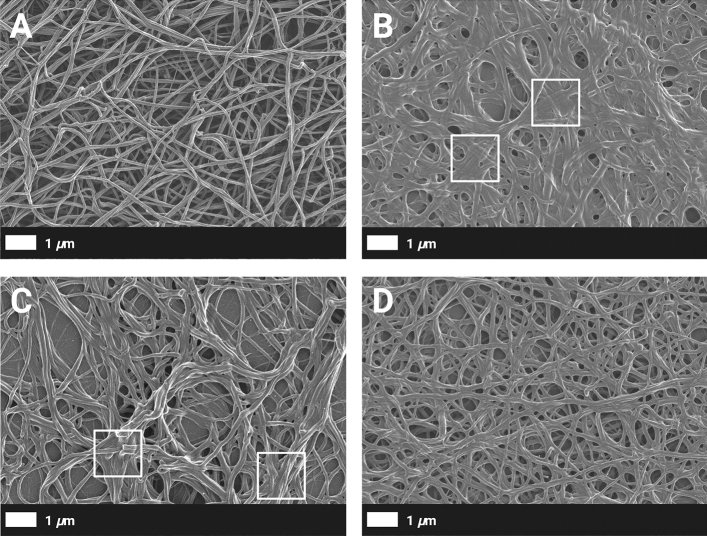
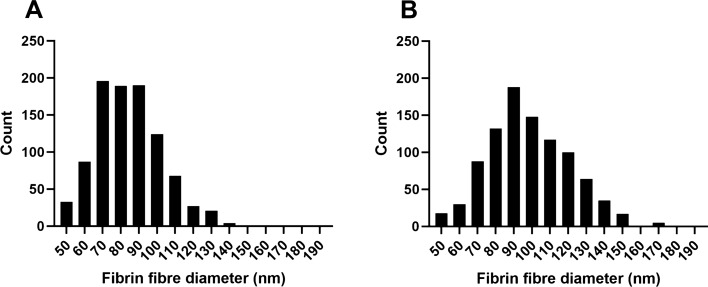
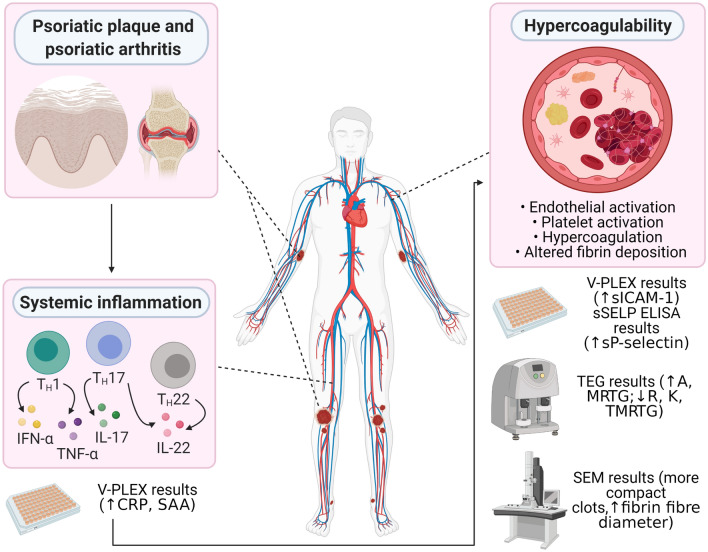
Psoriasis is a chronic, immune-mediated inflammatory skin disease, affecting approximately 2% of the general population, which can be accompanied by psoriatic arthritis (PsA). The condition has been associated with an increased cardiovascular burden. Hypercoagulability is a potential underlying mechanism that may contribute to the increased risk of major cardiovascular events in psoriatic individuals. Whole blood samples were collected from 20 PsA patients and 20 healthy individuals. The concentrations of inflammatory molecules (C-reactive protein, serum amyloid A, soluble intercellular adhesion molecule-1, soluble vascular cell adhesion molecule-1, and soluble P-selectin) were determined by enzyme-linked immunosorbent assays. In addition, clotting efficiency was evaluated by thromboelastography. The fibrin network architecture was also assessed by scanning electron microscopy. Elevated levels of circulating inflammatory molecules were significantly associated with the presence of psoriatic disease. Furthermore, an increased tendency towards thrombus formation was significantly predictive of disease presence. Scanning electron microscopy revealed that fibrin clots were denser in psoriatic individuals, compared to healthy controls, with an increased fibrin fibre diameter associated with psoriatic disease. Our results add to the accumulating evidence of the systemic nature of psoriasis and the subsequent risk of cardiovascular comorbidities, potentially due to an acquired hypercoagulability. We suggest that haemostatic function should be monitored carefully in psoriatic patients that present with severe disease, due to the pre-eminent risk of developing thrombotic complications.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
