

Novel vectors and approaches for gene therapy in liver diseases
- PMID: 34159305
- PMCID: PMC8203845
- DOI: 10.1016/j.jhepr.2021.100300
Novel vectors and approaches for gene therapy in liver diseases
Abstract
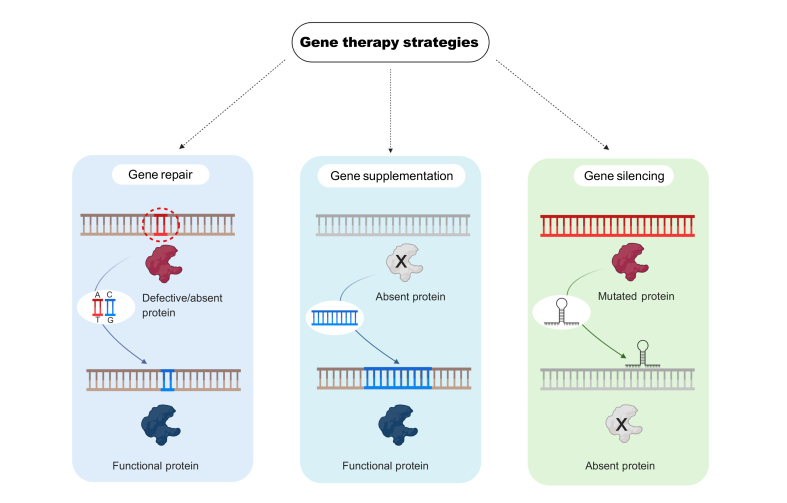
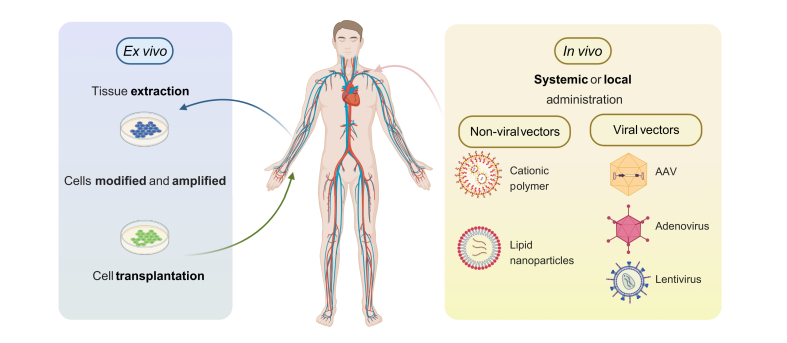
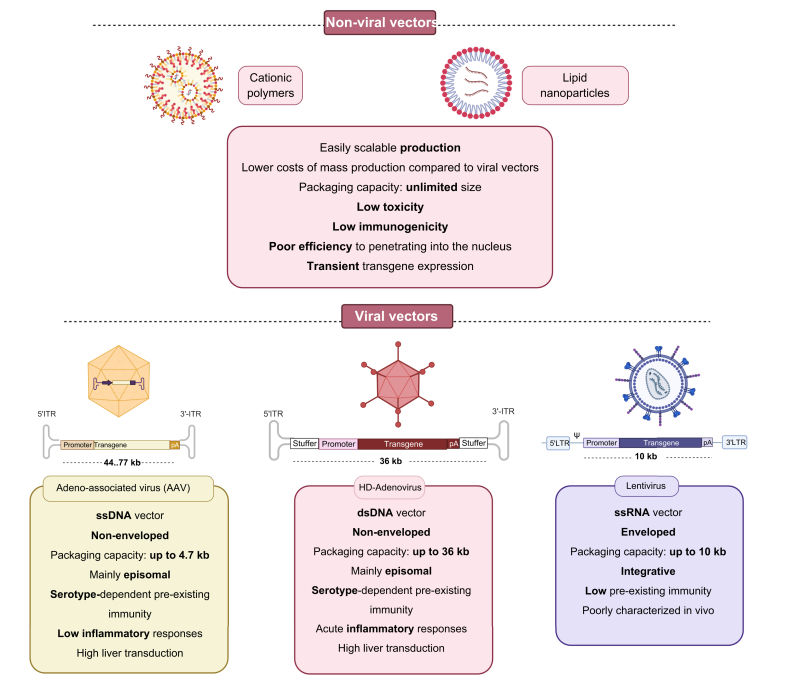
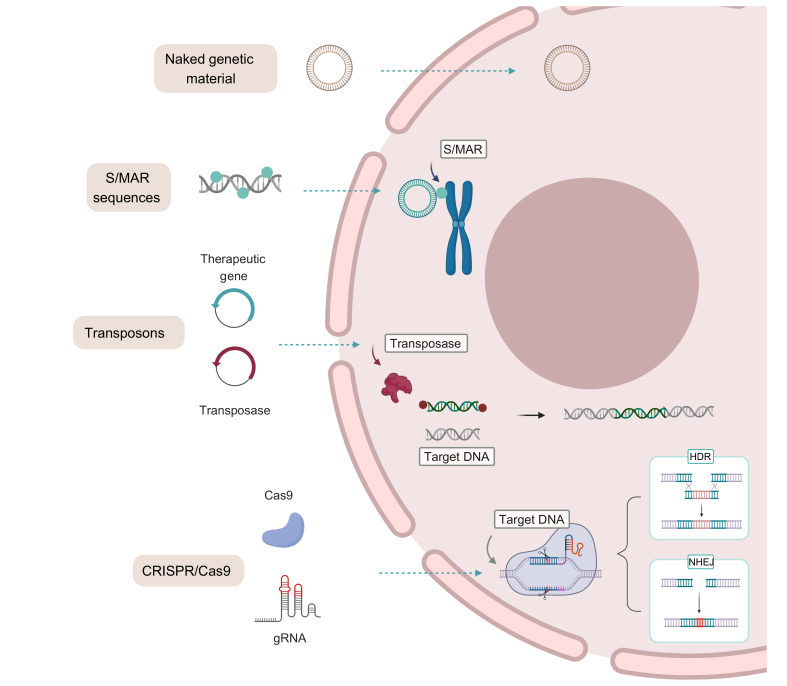
Gene therapy is becoming an increasingly valuable tool to treat many genetic diseases with no or limited treatment options. This is the case for hundreds of monogenic metabolic disorders of hepatic origin, for which liver transplantation remains the only cure. Furthermore, the liver contains 10-15% of the body's total blood volume, making it ideal for use as a factory to secrete proteins into the circulation. In recent decades, an expanding toolbox has become available for liver-directed gene delivery. Although viral vectors have long been the preferred approach to target hepatocytes, an increasing number of non-viral vectors are emerging as highly efficient vehicles for the delivery of genetic material. Herein, we review advances in gene delivery vectors targeting the liver and more specifically hepatocytes, covering strategies based on gene addition and gene editing, as well as the exciting results obtained with the use of RNA as a therapeutic molecule. Moreover, we will briefly summarise some of the limitations of current liver-directed gene therapy approaches and potential ways of overcoming them.
Keywords: AAT, α1-antitrypsin; AAV, adeno-associated virus; AHP, acute hepatic porphyrias; AIP, acute intermittent porphyria; ALAS1, aminolevulic synthase 1; APCs, antigen-presenting cells; ASGCT, American Society of Gene and Cell Therapy; ASGPR, asialoglycoprotein receptor; ASOs, antisense oligonucleotides; Ad, adenovirus; CBS, cystathionine β-synthase; CN, Crigel-Najjar; CRISPR, clustered regularly interspaced short palindromic repeats; CRISPR/Cas9, CRISPR associated protein 9; DSBs, double-strand breaks; ERT, enzyme replacement therapy; FH, familial hypercholesterolemia; FSP27, fat-specific protein 27; GO, glycolate oxidase; GSD1a, glycogen storage disorder 1a; GT, gene therapy; GUSB, β-glucuronidase; GalNAc, N-acetyl-D-galactosamine; HDAd, helper-dependent adenovirus; HDR, homology-directed repair; HT, hereditary tyrosinemia; HemA/B, haemophilia A/B; IDS, iduronate 2-sulfatase; IDUA, α-L-iduronidase; IMLD, inherited metabolic liver diseases; ITR, inverted terminal repetition; LDH, lactate dehydrogenase; LDLR, low-density lipoprotein receptor; LNP, Lipid nanoparticles; LTR, long terminal repeat; LV, lentivirus; MMA, methylmalonic acidemia; MPR, metabolic pathway reprograming; MPS type I, MPSI; MPS type VII, MPSVII; MPS, mucopolysaccharidosis; NASH, non-alcoholic steatohepatitis; NHEJ, non-homologous end joining; NHPs, non-human primates; Non-viral vectors; OLT, orthotopic liver transplantation; OTC, ornithine transcarbamylase; PA, propionic acidemia; PB, piggyBac; PCSK9, proprotein convertase subtilisin/kexin type 9; PEG, polyethylene glycol; PEI, polyethyleneimine; PFIC3, progressive familial cholestasis type 3; PH1, Primary hyperoxaluria type 1; PKU, phenylketonuria; RV, retrovirus; S/MAR, scaffold matrix attachment regions; SB, Sleeping Beauty; SRT, substrate reduction therapy; STK25, serine/threonine protein kinase 25; TALEN, transcription activator-like effector nucleases; TTR, transthyretin; UCD, urea cycle disorders; VLDLR, very-low-density lipoprotein receptor; WD, Wilson’s disease; ZFN, zinc finger nucleases; apoB/E, apolipoprotein B/E; dCas9, dead Cas9; efficacy; gene addition; gene editing; gene silencing; hepatocytes; immune response; lncRNA, long non-coding RNA; miRNAs, microRNAs; siRNA, small-interfering RNA; toxicity; viral vectors.
© 2021 The Authors.
Conflict of interest statement
NDW and GGA are Vivet Therapeutics employees and hold stock of the company. Please refer to the accompanying ICMJE disclosure forms for further details.
Figures
References
-
- American Society of Gene & Cell Therapy . 2019. Gene and cell therapy FAQs.https://www.asgct.org/education/more-resources/gene-and-cell-therapy-faqs
-
- Blaese R.M., Culver K.W., Miller A.D., Carter C.S., Fleisher T., Clerici M. T lymphocyte-directed gene therapy for ADA-SCID: initial trial results after 4 years. Science. 1995;270:475–480. - PubMed
-
- Bordignon C., Notarangelo L.D., Nobili N., Ferrari G., Casorati G., Panina P. Gene therapy in peripheral blood lymphocytes and bone marrow for ADA- immunodeficient patients. Science. 1995;270:470–475. - PubMed
-
- Raper S.E., Chirmule N., Lee F.S., Wivel N.A., Bagg A., Gao G.P. Fatal systemic inflammatory response syndrome in a ornithine transcarbamylase deficient patient following adenoviral gene transfer. Mol Genet Metab. 2003;80:148–158. - PubMed
-
- Hacein-Bey-Abina S., von Kalle C., Schmidt M., Le Deist F., Wulffraat N., McIntyre E. A serious adverse event after successful gene therapy for X-linked severe combined immunodeficiency. N Engl J Med. 2003;348:255–256. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
