

This is a preprint.
Subcutaneous REGEN-COV Antibody Combination in Early Asymptomatic SARS-CoV-2 Infection: A Randomized Clinical Trial
- PMID: 34159343
- PMCID: PMC8219113
- DOI: 10.1101/2021.06.14.21258569
Subcutaneous REGEN-COV Antibody Combination in Early Asymptomatic SARS-CoV-2 Infection: A Randomized Clinical Trial
Update in
-
Effect of Subcutaneous Casirivimab and Imdevimab Antibody Combination vs Placebo on Development of Symptomatic COVID-19 in Early Asymptomatic SARS-CoV-2 Infection: A Randomized Clinical Trial.JAMA. 2022 Feb 1;327(5):432-441. doi: 10.1001/jama.2021.24939. JAMA. 2022. PMID: 35029629 Free PMC article. Clinical Trial.
Abstract
Importance: Easy-to-administer antiviral treatments may be used to prevent progression from asymptomatic infection to COVID-19 and to reduce viral carriage.
Objective: Evaluate the efficacy and safety of subcutaneous casirivimab and imdevimab antibody combination (REGEN-COV) to prevent progression from early asymptomatic SARS-CoV-2 infection to COVID-19.
Design: Randomized, double-blind, placebo-controlled, phase 3 study that enrolled asymptomatic close contacts living with a SARS-CoV-2-infected household member (index case). Participants who were SARS-CoV-2 RT-qPCR-positive at baseline were included in the analysis reported here.
Setting: Multicenter trial conducted at 112 sites in the United States, Romania, and Moldova.
Participants: Asymptomatic individuals ≥12 years of age were eligible if identified within 96 hours of collection of the index case's positive SARS-CoV-2 test sample.
Interventions: A total of 314 asymptomatic, SARS-CoV-2 RT-qPCR-positive individuals living with an infected household contact were randomized 1:1 to receive a single dose of subcutaneous REGEN-COV 1200mg (n=158) or placebo (n=156).
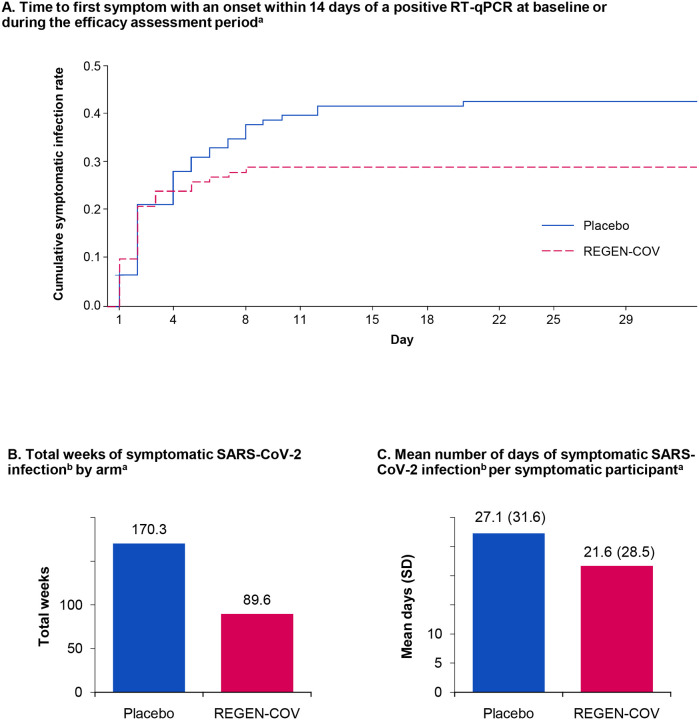
Main outcomes and measures: The primary endpoint was the proportion of participants who developed symptomatic COVID-19 during the 28-day efficacy assessment period. The key secondary efficacy endpoints were the number of weeks of symptomatic SARS-CoV-2 infection and the number of weeks of high viral load (>4 log10 copies/mL). Safety was assessed in all treated participants.
Results: Subcutaneous REGEN-COV 1200mg significantly prevented progression from asymptomatic to symptomatic disease compared with placebo (31.5% relative risk reduction; 29/100 [29.0%] vs 44/104 [42.3%], respectively; P=.0380). REGEN-COV reduced the overall population burden of high-viral load weeks (39.7% reduction vs placebo; 48 vs 82 total weeks; P=.0010) and of symptomatic weeks (45.3% reduction vs placebo; 89.6 vs 170.3 total weeks; P=.0273), the latter corresponding to an approximately 5.6-day reduction in symptom duration per symptomatic participant. Six placebo-treated participants had a COVID-19-related hospitalization or ER visit versus none for those receiving REGEN-COV. The proportion of participants receiving placebo who had ≥1 treatment-emergent adverse events was 48.1% compared with 33.5% for those receiving REGEN-COV, including events related (39.7% vs 25.8%, respectively) or not related (16.0% vs 11.0%, respectively) to COVID-19.
Conclusions and relevance: Subcutaneous REGEN-COV 1200mg prevented progression from asymptomatic SARS-CoV-2 infection to COVID-19, reduced the duration of high viral load and symptoms, and was well tolerated.
Trial registration: ClinicalTrials.gov Identifier, NCT04452318.
Figures

References
-
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Accessed September 14, 2021. https://covid19.who.int/table.
-
- Centers for Disease Control and Prevention. Clinical questions about COVID-19: questions and answers. Transmission. Accessed April 23, 2021. https://www.cdc.gov/coronavirus/2019-ncov/hcp/faq.html#Transmission
Publication types
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous