

Perioperative and short-term oncological outcomes following laparoscopic versus open pancreaticoduodenectomy after learning curve in the past 10 years: a systematic review and meta-analysis
- PMID: 34164310
- PMCID: PMC8184374
- DOI: 10.21037/gs-20-916
Perioperative and short-term oncological outcomes following laparoscopic versus open pancreaticoduodenectomy after learning curve in the past 10 years: a systematic review and meta-analysis
Abstract
Background: To compare perioperative and short-term oncologic outcomes of laparoscopic pancreaticoduodenectomy (LPD) to open pancreaticoduodenectomy (OPD) using data from large-scale retrospective cohorts and randomized controlled trials (RCTs) in the last 10 years.
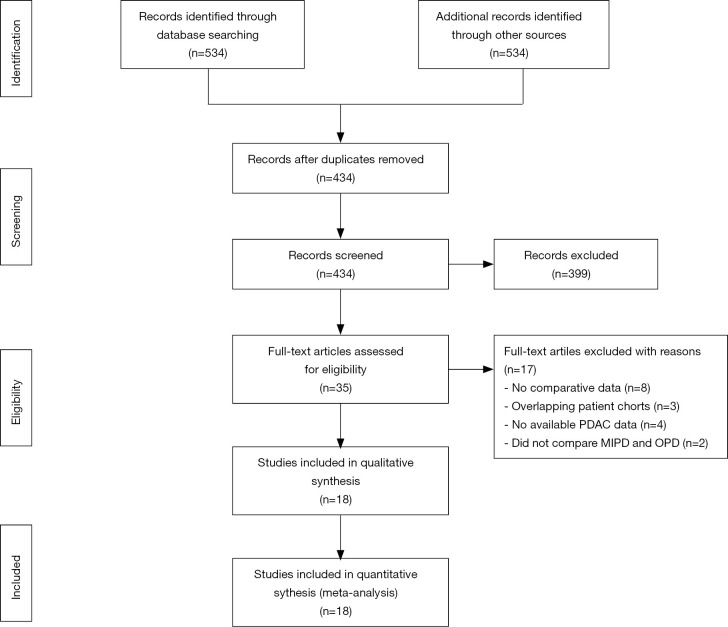
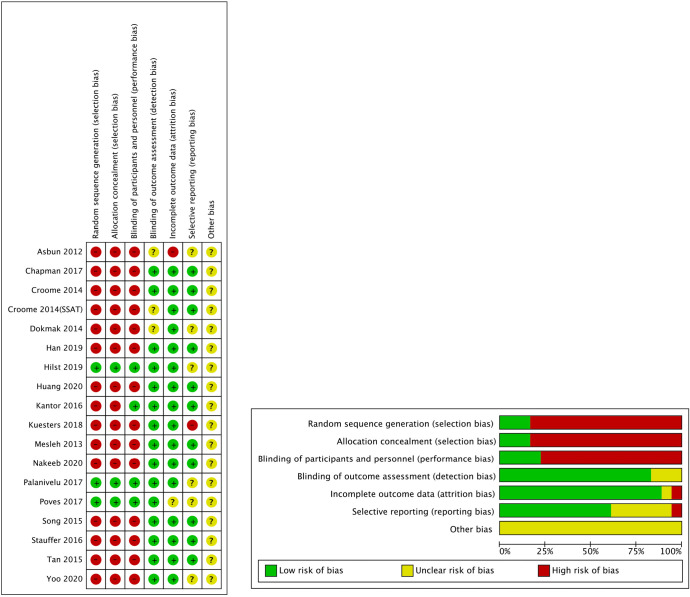
Methods: A meta-analysis to assess the safety and feasibility of LDP and OPD registered with PROSPERO: (CRD42020218080) was performed according to the PRISMA guidelines. Studies comparing LPD with OPD published between January 2010 and October 2020 were included; only clinical studies reporting more than 30 cases for each operation were included. Two authors performed data extraction and quality assessment independently. The primary endpoint was operative times, blood loss, and 90 days mortality. Secondary endpoints included reoperation, length of hospital stay (LOS), morbidity, Clavien-Dindo ≥3 complications, postoperative pancreatic fistula (POPF), blood transfusion, delayed gastric emptying (DGE), postpancreatectomy hemorrhage (PPH), and oncologic outcomes (R0-resection, lymph node dissection).
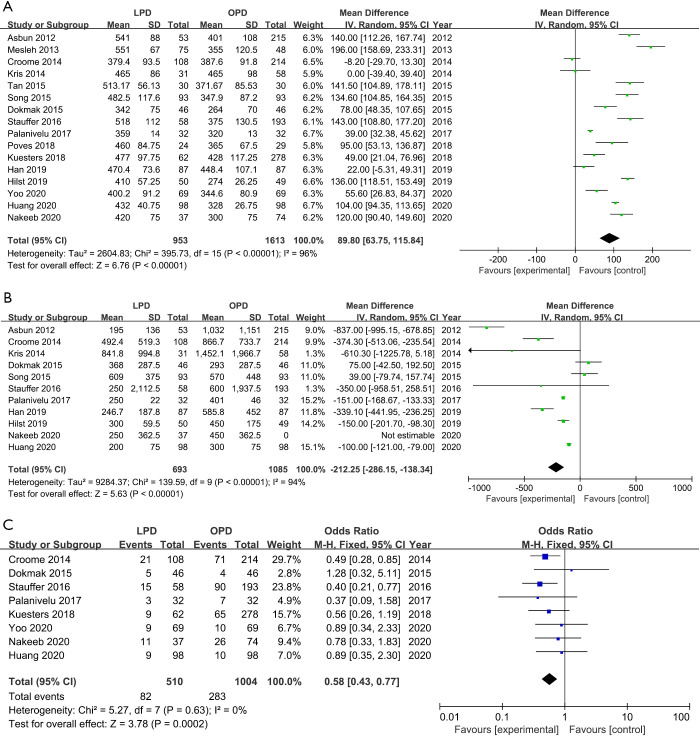
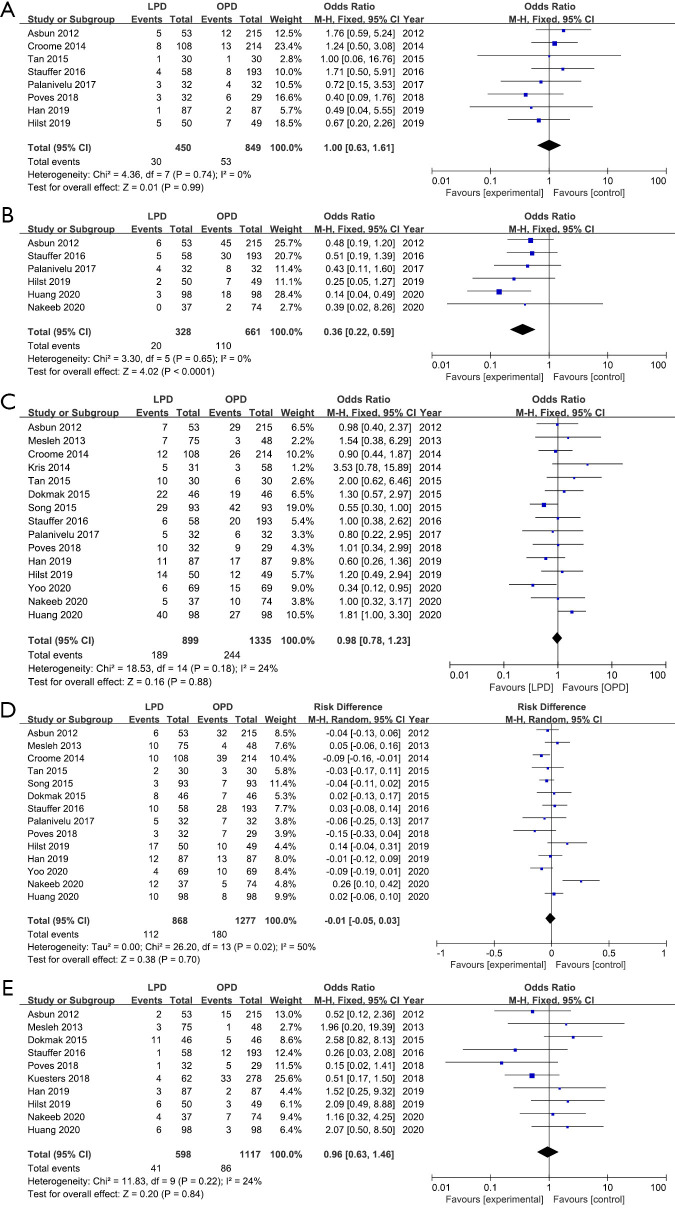
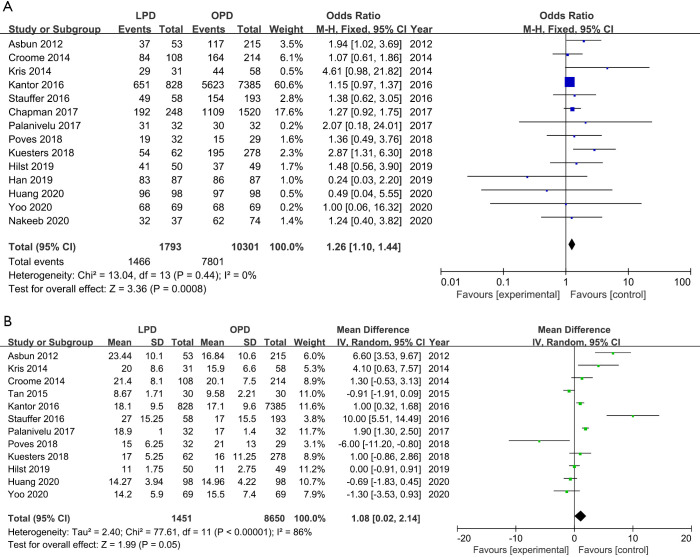
Results: Overall, the final analysis included 15 retrospective cohorts and 3 RCTs comprising 12,495 patients (2,037 and 10,458 patients underwent LPD and OPD). It seems OPD has more lymph nodes harvested but no significant differences [weighted mean difference (WMD): 1.08; 95% confidence interval (CI): 0.02 to 2.14; P=0.05]. Nevertheless, compared with OPD, LPD was associated with a higher R0 resection rate [odds ratio (OR): 1.26; 95% CI: 1.10-1.44; P=0.0008] and longer operative time (WMD: 89.80 min; 95% CI: 63.75-115.84; P<0.00001), patients might benefit from lower rate of wound infection (OR: 0.36; 95% CI: 0.33-0.59; P<0.0001), much less blood loss (WMD: -212.25 mL; 95% CI: -286.15 to -138.14; P<0.00001) and lower blood transfusion rate (OR: 0.58; 95% CI: 0.43-0.77; P=0.0002) and shorter LOS (WMD: -1.63 day; 95% CI: -2.73 to -0.51; P=0.004). No significant differences in 90-day mortality, overall morbidity, Clavien-Dindo ≥3 complications, reoperation, POPF, DGE and PPH between LPD and OPD.
Conclusions: Our study suggests that after learning curve, LPD is a safe and feasible alternative to OPD as it provides similar perioperative and acceptable oncological outcomes when compared with OPD.
Keywords: Pancreatic cancer; laparoscopic pancreaticoduodenectomy (LPD); meta-analysis; open pancreaticoduodenectomy (OPD).
2021 Gland Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/gs-20-916). The authors have no conflicts of interest to declare.
Figures


Similar articles
-
Laparoscopic vs. Open Pancreaticoduodenectomy After Learning Curve: A Systematic Review and Meta-Analysis of Single-Center Studies.Front Surg. 2021 Sep 10;8:715083. doi: 10.3389/fsurg.2021.715083. eCollection 2021. Front Surg. 2021. Retraction in: Front Surg. 2022 Jul 26;9:988654. doi: 10.3389/fsurg.2022.988654. PMID: 34568416 Free PMC article. Retracted.
-
Laparoscopic Pancreaticoduodenectomy Versus Conventional Open Approach for Patients With Pancreatic Duct Adenocarcinoma: An Up-to-Date Systematic Review and Meta-Analysis.Front Oncol. 2021 Oct 27;11:749140. doi: 10.3389/fonc.2021.749140. eCollection 2021. Front Oncol. 2021. PMID: 34778064 Free PMC article.
-
Laparoscopic versus open pancreaticoduodenectomy for pancreatic and periampullary tumor: A meta-analysis of randomized controlled trials and non-randomized comparative studies.Front Oncol. 2023 Jan 25;12:1093395. doi: 10.3389/fonc.2022.1093395. eCollection 2022. Front Oncol. 2023. PMID: 36761416 Free PMC article.
-
Is total laparoscopic pancreaticoduodenectomy superior to open procedure? A meta-analysis.World J Gastroenterol. 2019 Oct 7;25(37):5711-5731. doi: 10.3748/wjg.v25.i37.5711. World J Gastroenterol. 2019. PMID: 31602170 Free PMC article.
-
Laparoscopic Versus Open Pancreaticoduodenectomy: A Systematic Review and Meta-analysis of Randomized Controlled Trials.Ann Surg. 2020 Jan;271(1):54-66. doi: 10.1097/SLA.0000000000003309. Ann Surg. 2020. PMID: 30973388
Cited by
-
Is robotic distal pancreatectomy better than laparoscopic distal pancreatectomy after the learning curve? A systematic review and meta-analysis.Front Oncol. 2022 Aug 29;12:954227. doi: 10.3389/fonc.2022.954227. eCollection 2022. Front Oncol. 2022. PMID: 36106111 Free PMC article.
-
Glucose Regulation after Partial Pancreatectomy: A Comparison of Pancreaticoduodenectomy and Distal Pancreatectomy in the Short and Long Term.Diabetes Metab J. 2023 Sep;47(5):703-714. doi: 10.4093/dmj.2022.0205. Epub 2023 Jun 22. Diabetes Metab J. 2023. PMID: 37349082 Free PMC article.
-
An analysis of risk factors for clinically relevant pancreatic fistulas after laparoscopic pancreaticoduodenectomy.Medicine (Baltimore). 2023 May 19;102(20):e33759. doi: 10.1097/MD.0000000000033759. Medicine (Baltimore). 2023. PMID: 37335734 Free PMC article.
-
Causes and predictors of unplanned reoperations within 30 days post laparoscopic pancreaticoduodenectomy: a comprehensive analysis.Front Oncol. 2024 Aug 23;14:1464450. doi: 10.3389/fonc.2024.1464450. eCollection 2024. Front Oncol. 2024. PMID: 39257554 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Miscellaneous