

Pulmonary embolism in patients with COVID-19: incidence, risk factors, clinical characteristics, and outcome
- PMID: 34164664
- PMCID: PMC8344714
- DOI: 10.1093/eurheartj/ehab314
Pulmonary embolism in patients with COVID-19: incidence, risk factors, clinical characteristics, and outcome
Abstract
Aims: We investigated the incidence, risk factors, clinical characteristics, and outcomes of pulmonary embolism (PE) in patients with COVID-19 attending emergency departments (EDs), before hospitalization.
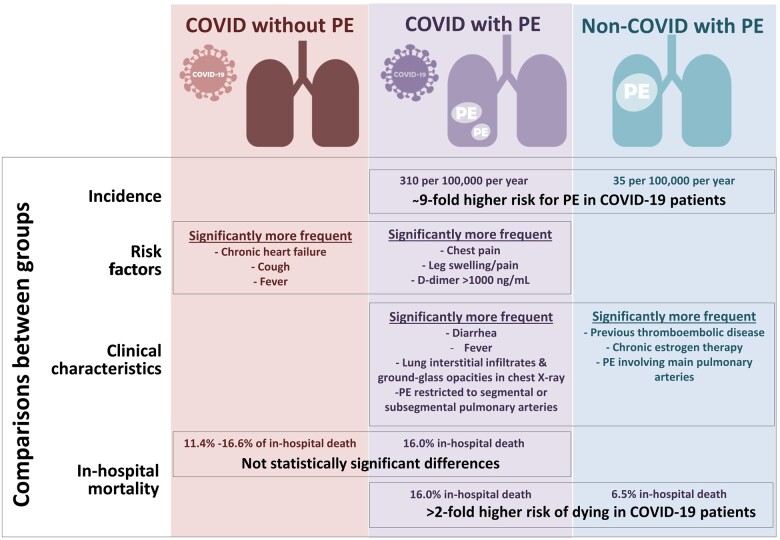
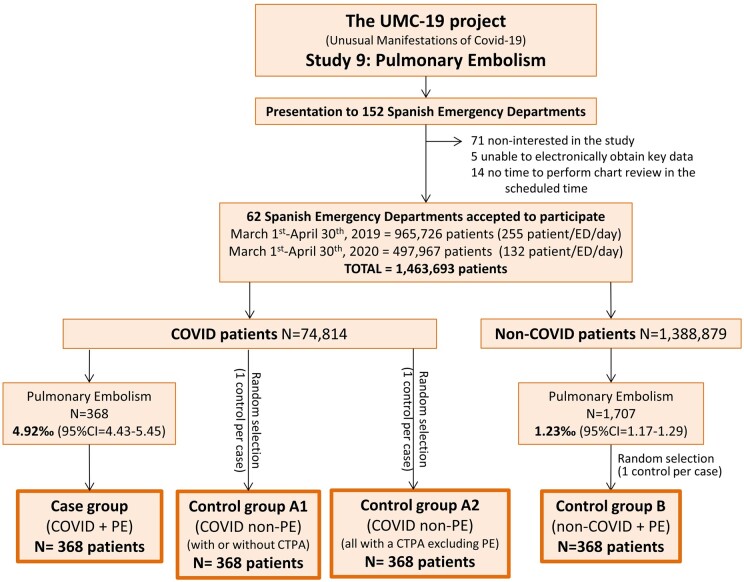
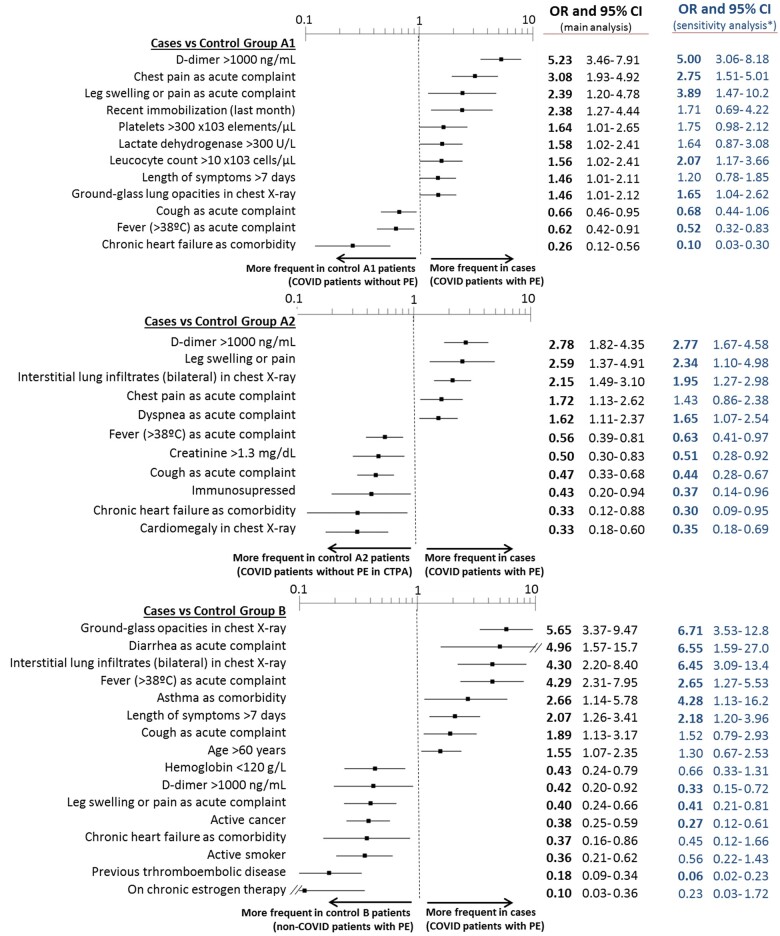
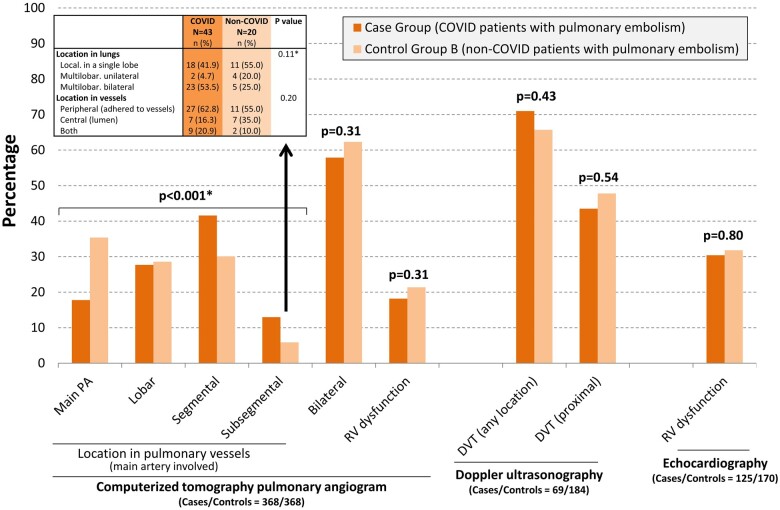
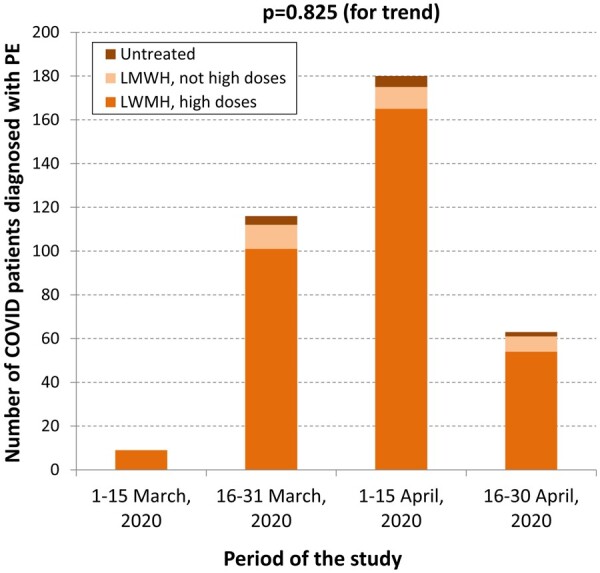
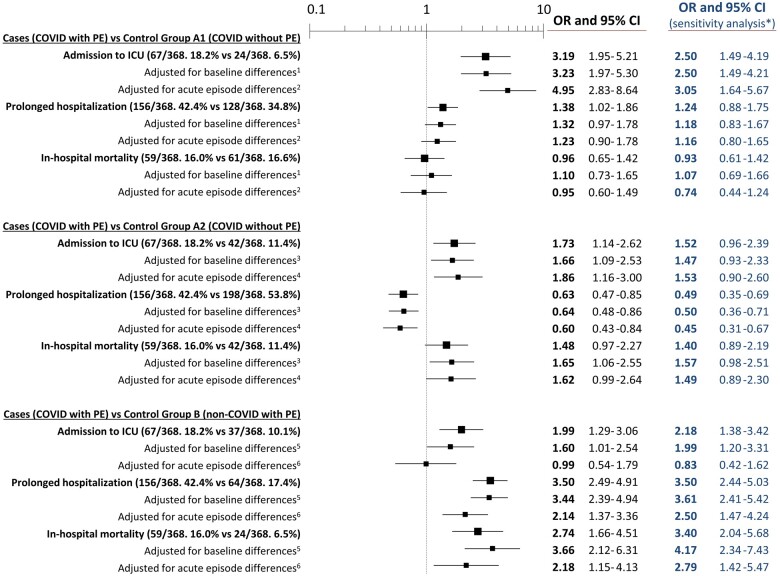
Methods and results: We retrospectively reviewed all COVID-19 patients diagnosed with PE in 62 Spanish EDs (20% of Spanish EDs, case group) during the first COVID-19 outbreak. COVID-19 patients without PE and non-COVID-19 patients with PE were included as control groups. Adjusted comparisons for baseline characteristics, acute episode characteristics, and outcomes were made between cases and randomly selected controls (1:1 ratio). We identified 368 PE in 74 814 patients with COVID-19 attending EDs (4.92‰). The standardized incidence of PE in the COVID-19 population resulted in 310 per 100 000 person-years, significantly higher than that observed in the non-COVID-19 population [35 per 100 000 person-years; odds ratio (OR) 8.95 for PE in the COVID-19 population, 95% confidence interval (CI) 8.51-9.41]. Several characteristics in COVID-19 patients were independently associated with PE, the strongest being D-dimer >1000 ng/mL, and chest pain (direct association) and chronic heart failure (inverse association). COVID-19 patients with PE differed from non-COVID-19 patients with PE in 16 characteristics, most directly related to COVID-19 infection; remarkably, D-dimer >1000 ng/mL, leg swelling/pain, and PE risk factors were significantly less present. PE in COVID-19 patients affected smaller pulmonary arteries than in non-COVID-19 patients, although right ventricular dysfunction was similar in both groups. In-hospital mortality in cases (16.0%) was similar to COVID-19 patients without PE (16.6%; OR 0.96, 95% CI 0.65-1.42; and 11.4% in a subgroup of COVID-19 patients with PE ruled out by scanner, OR 1.48, 95% CI 0.97-2.27), but higher than in non-COVID-19 patients with PE (6.5%; OR 2.74, 95% CI 1.66-4.51). Adjustment for differences in baseline and acute episode characteristics and sensitivity analysis reported very similar associations.
Conclusions: PE in COVID-19 patients at ED presentation is unusual (about 0.5%), but incidence is approximately ninefold higher than in the general (non-COVID-19) population. Moreover, risk factors and leg symptoms are less frequent, D-dimer increase is lower and emboli involve smaller pulmonary arteries. While PE probably does not increase the mortality of COVID-19 patients, mortality is higher in COVID-19 than in non-COVID-19 patients with PE.
Keywords: COVID-19; Clinical characteristics; Incidence; Outcome; Pulmonary embolism; Risk factors; SARS-CoV-2.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author(s) 2021. For permissions, please email: journals.permissions@oup.com.
Figures
Comment in
-
Hypercoagulability and thrombosis in COVID-19: a modifiable cause for mortality?Eur Heart J. 2021 Aug 31;42(33):3143-3145. doi: 10.1093/eurheartj/ehab417. Eur Heart J. 2021. PMID: 34254136 Free PMC article. No abstract available.
References
-
- Wiersinga WJ, Rhodes A, Cheng AC, Peacock SJ, Prescott HC.. Pathophysiology, transmission, diagnosis, and treatment of coronavirus disease 2019 (COVID-19): a review. JAMA 2020;324:782–793. - PubMed
-
- Fauvel C, Weizman O, Trimaille A, Mika D, Pommier T, Pace N, Douair A, Barbin E, Fraix A, Bouchot O, Benmansour O, Godeau G, Mecheri Y, Lebourdon R, Yvorel C, Massin M, Leblon T, Chabbi C, Cugney E, Benabou L, Aubry M, Chan C, Boufoula I, Barnaud C, Bothorel L, Duceau B, Sutter W, Waldmann V, Bonnet G, Cohen A, Pezel T, Critical Covid-19 France Investigators. Pulmonary embolism in COVID-19 patients: a French multicentre cohort study. Eur Heart J 2020;41:3058–3068. - PMC - PubMed
-
- Ministry of Health. Spanish Government. COVID-19 Geographical Distribution. (https://cnecovid.isciii.es/covid19/#niveles-de-gravedad (accessed 1 June 2020).
-
- Miró O, González Del Castillo J.. Collaboration among Spanish emergency departments to promote research: on the creation of the SIESTA (Spanish Investigators in Emergency Situations TeAm) network and the coordination of the UMC-19 (Unusual Manifestations of COVID-19) macroproject. Emergencias 2020;32:269–277. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
