

Cat at home? Cat scratch disease with atypical presentations and aggressive radiological findings mimicking sarcoma, a potential diagnostic pitfall
- PMID: 34165046
- PMCID: PMC8635669
- DOI: 10.1080/17453674.2021.1941624
Cat at home? Cat scratch disease with atypical presentations and aggressive radiological findings mimicking sarcoma, a potential diagnostic pitfall
Abstract
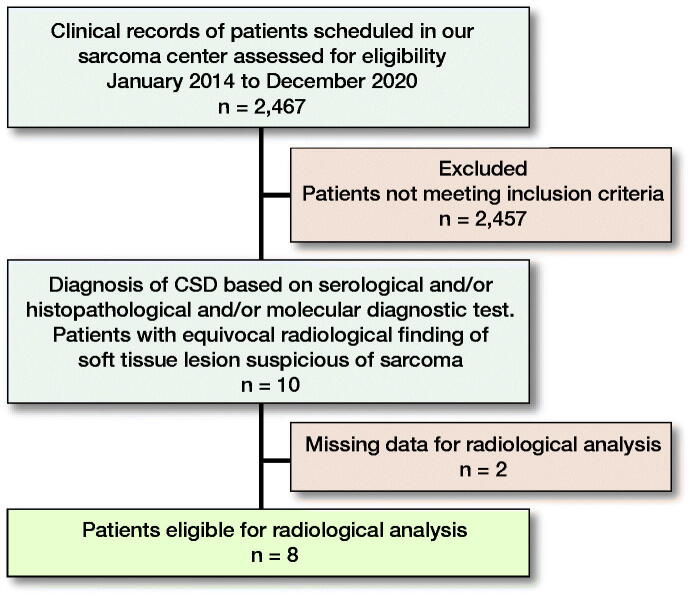
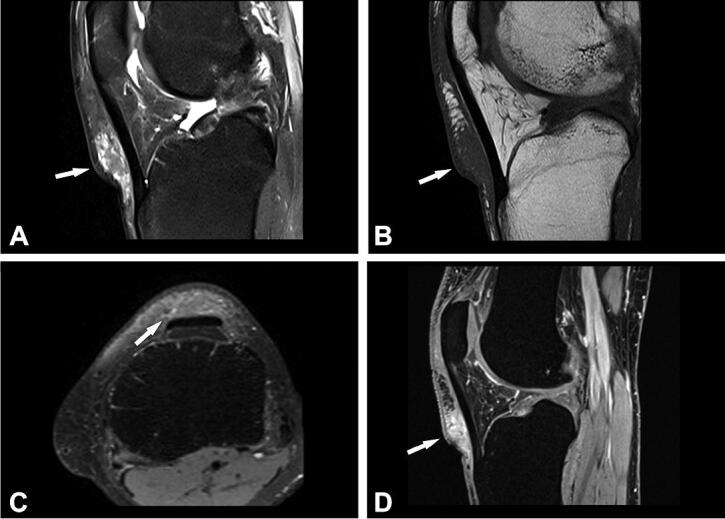
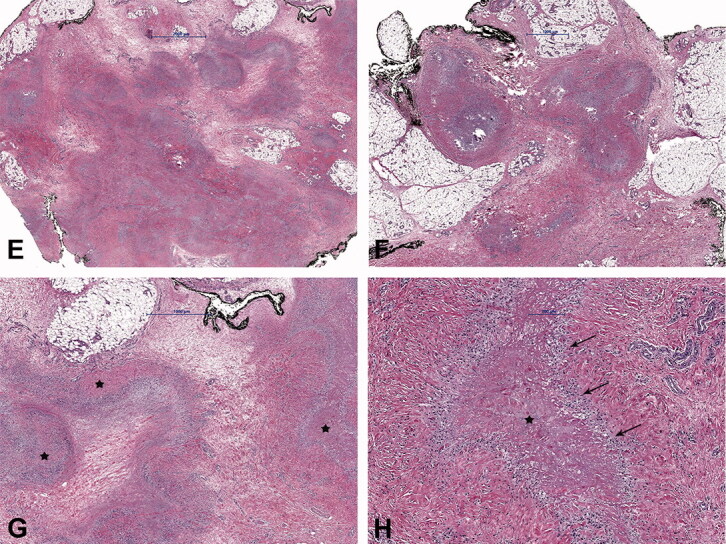
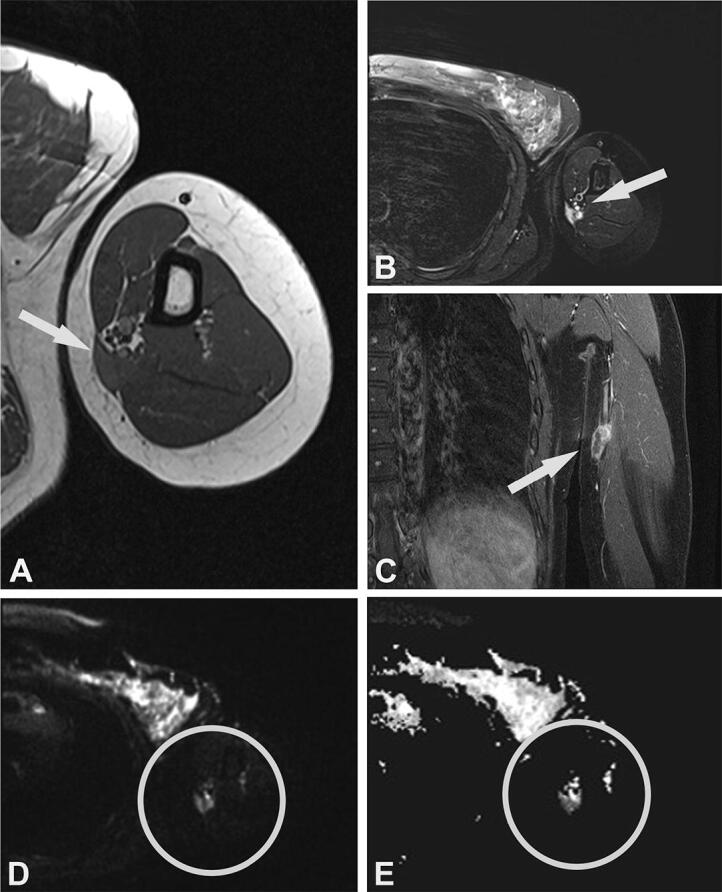
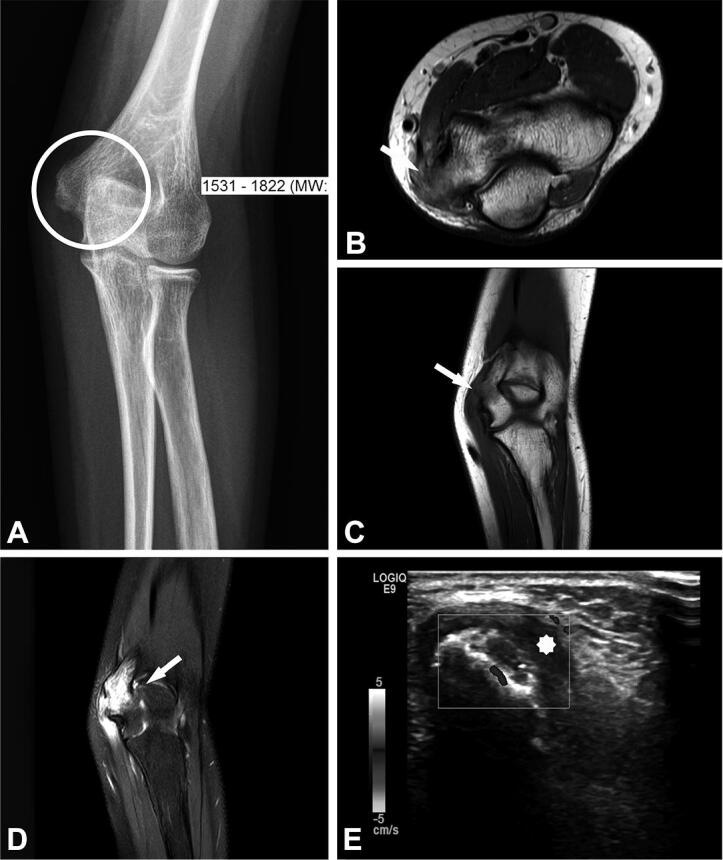
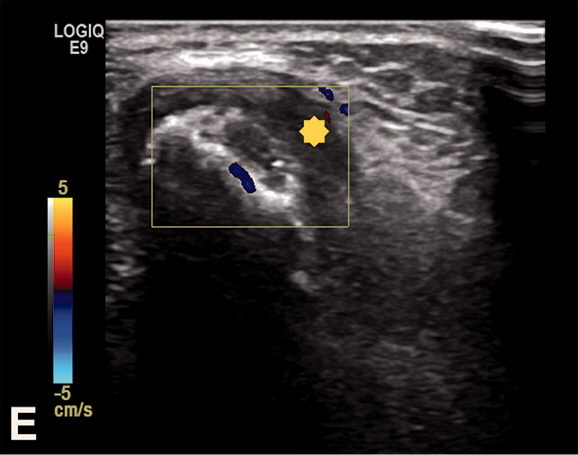
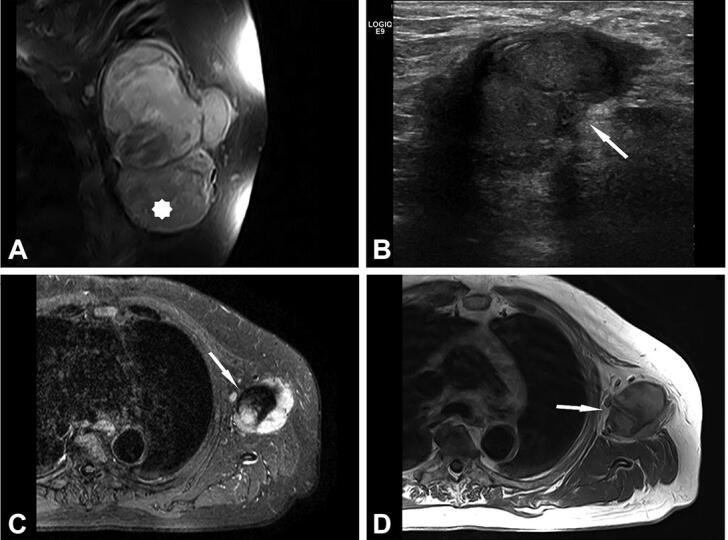
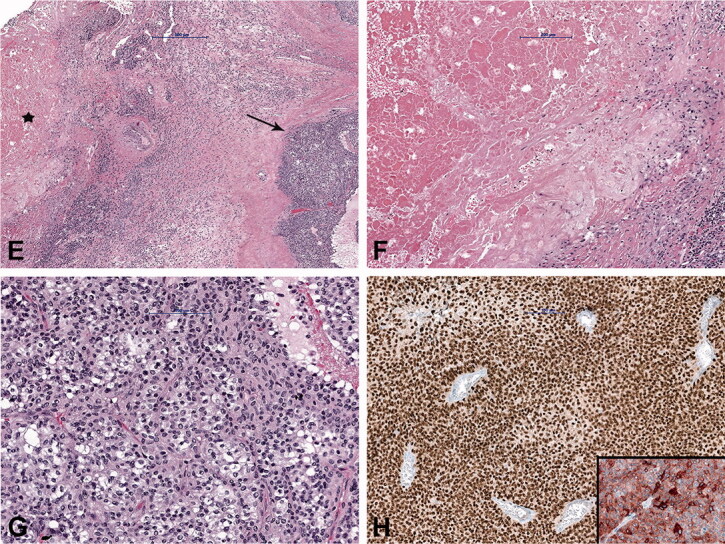
Background and purpose - Cat scratch disease (CSD) is a self-limiting disease caused by Bartonella (B.) henselae. It is characterized by granulomatous infection, most frequently involving lymph nodes. However, it can present with atypical symptoms including musculoskeletal manifestations, posing a diagnostic challenge. We describe the prevalence and demographics of CSD cases referred to a sarcoma center, and describe the radiological, histological, and molecular findings.Patients and methods - Our cohort comprised 10 patients, median age 27 years (12-74) with clinical and radiological findings suspicious of sarcoma.Results - 7 cases involved the upper extremities, and 1 case each involved the axilla, groin, and knee. B. henselae was found in 6 cases tested using polymerase chain reaction and serology in 5 cases. 9 cases were soft tissue lesions and 1 lesion involved the bone. 1 patient had concomitant CSD with melanoma metastasis in enlarged axillary lymph nodes. On MRI, 5 soft tissue lesions were categorized as probably inflammatory. In 3 cases, with still detectable lymph node structure and absent or initial liquefaction, the differential diagnosis included lymph node metastasis. A sarcoma diagnosis was suggested in 4 cases. The MRI imaging features of the bone lesion were suspicious of a bone tumor or osteomyelitis.Interpretation - Atypical imaging findings cause a diagnostic challenge and the differential diagnosis includes malignant neoplasms (such as sarcoma or carcinoma metastasis) and other infections. The distinction between these possibilities is crucial for treatment and prognosis.
Figures
Similar articles
-
Cat scratch disease--heterogeneous in clinical presentation: five unusual cases of an infection caused by Bartonella henselae.Klin Padiatr. 2010 Mar;222(2):73-8. doi: 10.1055/s-0029-1233488. Epub 2009 Sep 29. Klin Padiatr. 2010. PMID: 19790029
-
Role of magnetic resonance imaging and scintigraphy in the diagnosis and follow-up of osteomyelitis in cat-scratch disease.J Paediatr Child Health. 2007 Jul-Aug;43(7-8):568-70. doi: 10.1111/j.1440-1754.2007.01141.x. J Paediatr Child Health. 2007. PMID: 17635689
-
Detection of Bartonella henselae DNA by two different PCR assays and determination of the genotypes of strains involved in histologically defined cat scratch disease.J Clin Microbiol. 1999 Apr;37(4):993-7. doi: 10.1128/JCM.37.4.993-997.1999. J Clin Microbiol. 1999. PMID: 10074515 Free PMC article.
-
Bartonella henselae infections in solid organ transplant recipients: report of 5 cases and review of the literature.Medicine (Baltimore). 2012 Mar;91(2):111-121. doi: 10.1097/MD.0b013e31824dc07a. Medicine (Baltimore). 2012. PMID: 22391473 Review.
-
Multifocal pelvic osteomyelitis in a child associated with cat-scratch disease: a case report and review of the literature.Paediatr Int Child Health. 2019 Nov;39(4):290-293. doi: 10.1080/20469047.2018.1476304. Epub 2018 Aug 10. Paediatr Int Child Health. 2019. PMID: 30092749
Cited by
-
Impact of Educational Program on Critical Care Nurses' Knowledge of ICU Delirium: A Quasi-Experimental Study.Med Arch. 2023 Feb;77(1):56-63. doi: 10.5455/medarh.2023.77.56-63. Med Arch. 2023. PMID: 36919128 Free PMC article.
-
Cat-Scratch Lymphadenitis Presenting with Right Upper Arm and Axillary Masses: a Case Report Mimicking Lymphoma and Potential Diagnostic Pitfall.Med Arch. 2022 Dec;76(6):480-483. doi: 10.5455/medarh.2022.76.480-483. Med Arch. 2022. PMID: 36937617 Free PMC article.
-
Cat-scratch disease mimicking soft tissue sarcoma in a pediatric patient.Radiol Case Rep. 2025 Mar 8;20(5):2248-2252. doi: 10.1016/j.radcr.2025.01.071. eCollection 2025 May. Radiol Case Rep. 2025. PMID: 40129778 Free PMC article.
References
-
- Baranowski K, Cat Huang B.. scratch disease. In: StatPearls. Treasure Island, FL: StatPearls Publishing LLC; 2020. - PubMed
-
- Bernard S A, Walker E A, Carroll J F, Klassen-Fischer M, Murphey M D.. Epitrochlear cat scratch disease: unique imaging features allowing differentiation from other soft tissue masses of the medial arm. Skeletal Radiol 2016; 45(9): 1227–34. - PubMed
-
- Carithers H A. Cat-scratch disease: an overview based on a study of 1,200 patients. Am J Dis Child 1985; 139(11): 1124–33. - PubMed
-
- Colman M W, Lozano-Calderon S, Raskin K A, Hornicek F J, Gebhardt M.. Non-neoplastic soft tissue masses that mimic sarcoma. Orthop Clin North Am 2014; 45(2): 245–55. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous