

Association Between an Increase in Serum Sodium and In-Hospital Mortality in Critically Ill Patients
- PMID: 34166287
- PMCID: PMC8594512
- DOI: 10.1097/CCM.0000000000005173
Association Between an Increase in Serum Sodium and In-Hospital Mortality in Critically Ill Patients
Abstract
Objectives: In critically ill patients, dysnatremia is common, and in these patients, in-hospital mortality is higher. It remains unknown whether changes of serum sodium after ICU admission affect mortality, especially whether normalization of mild hyponatremia improves survival.
Design: Retrospective cohort study.
Setting: Ten Dutch ICUs between January 2011 and April 2017.
Patients: Adult patients were included if at least one serum sodium measurement within 24 hours of ICU admission and at least one serum sodium measurement 24-48 hours after ICU admission were available.
Interventions: None.
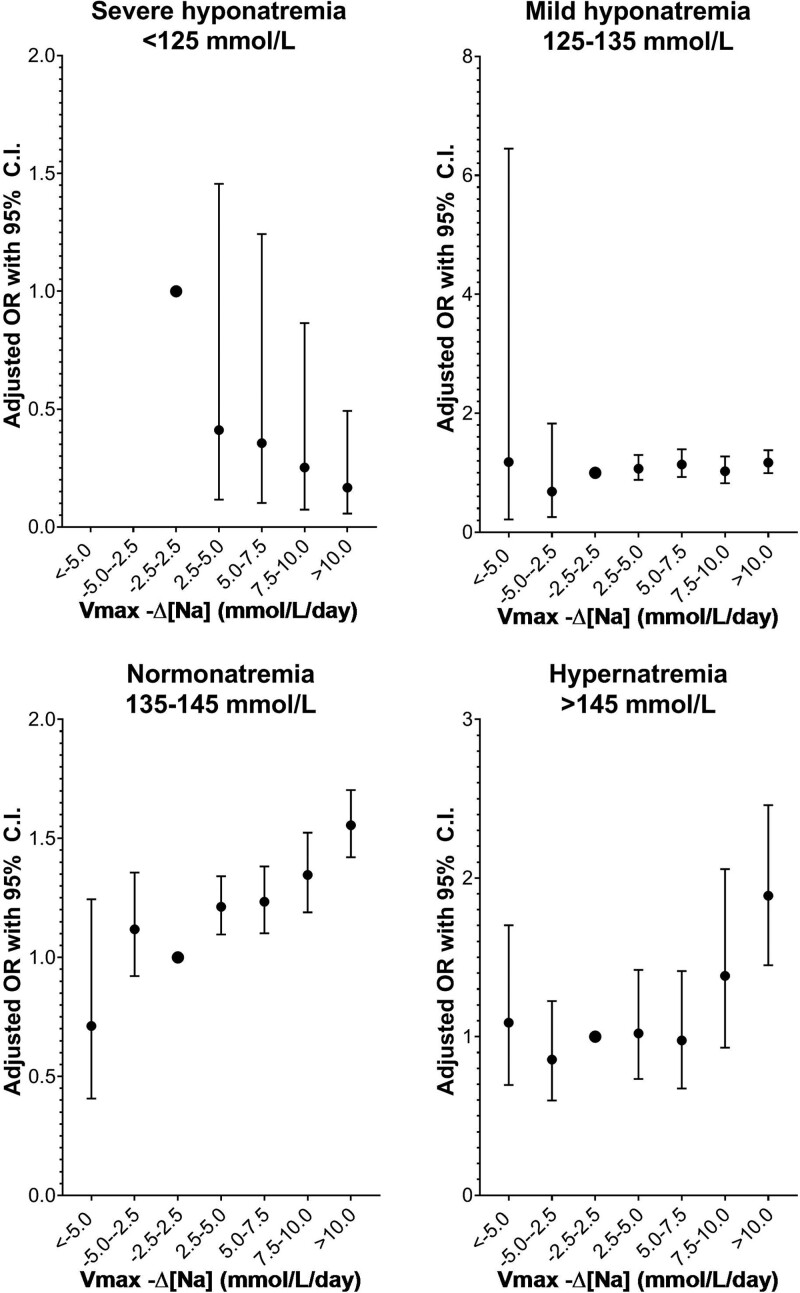
Measurements and main results: A logistic regression model adjusted for age, sex, and Acute Physiology and Chronic Health Evaluation-IV-predicted mortality was used to assess the difference between mean of sodium measurements 24-48 hours after ICU admission and first serum sodium measurement at ICU admission (Δ48 hr-[Na]) and in-hospital mortality. In total, 36,660 patients were included for analysis. An increase in serum sodium was independently associated with a higher risk of in-hospital mortality in patients admitted with normonatremia (Δ48 hr-[Na] 5-10 mmol/L odds ratio: 1.61 [1.44-1.79], Δ48 hr-[Na] > 10 mmol/L odds ratio: 4.10 [3.20-5.24]) and hypernatremia (Δ48 hr-[Na] 5-10 mmol/L odds ratio: 1.47 [1.02-2.14], Δ48 hr-[Na] > 10 mmol/L odds ratio: 8.46 [3.31-21.64]). In patients admitted with mild hyponatremia and Δ48 hr-[Na] greater than 5 mmol/L, no significant difference in hospital mortality was found (odds ratio, 1.11 [0.99-1.25]).
Conclusions: An increase in serum sodium in the first 48 hours of ICU admission was associated with higher in-hospital mortality in patients admitted with normonatremia and in patients admitted with hypernatremia.
Copyright © 2021 by the Society of Critical Care Medicine and Wolters Kluwer Health, Inc. All Rights Reserved.
Conflict of interest statement
Drs. Termorshuizen’s and de Keizer’s institutions received funding from the National Intensive Care Evaluation Foundation. Dr. Termorshuizen received funding from the Mental Health Care Institute, Rivierduinen, Leiden. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures

Comment in
-
Sodium Rising: Deciphering the Code.Crit Care Med. 2021 Dec 1;49(12):2143-2145. doi: 10.1097/CCM.0000000000005222. Crit Care Med. 2021. PMID: 34793381 No abstract available.
-
What Is the Abnormal Serum Sodium to Be Associated With Mortality in Critically Ill?Crit Care Med. 2022 Jun 1;50(6):e596-e597. doi: 10.1097/CCM.0000000000005496. Epub 2022 May 19. Crit Care Med. 2022. PMID: 35612449 No abstract available.
References
-
- Dasta J, Waikar SS, Xie L, et al. Patterns of treatment and correction of hyponatremia in intensive care unit patients. J Crit Care. 2015; 30:1072–1079 - PubMed
-
- Sakr Y, Rother S, Ferreira AM, et al. Fluctuations in serum sodium level are associated with an increased risk of death in surgical ICU patients. Crit Care Med. 2013; 41:133–142 - PubMed
-
- Pokaharel M, Block CA. Dysnatremia in the ICU. Curr Opin Crit Care. 2011; 17:581–593 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
