

HIV-1 Recent Infection Testing Algorithm With Antiretroviral Drug Detection to Improve Accuracy of Incidence Estimates
- PMID: 34166315
- PMCID: PMC8630595
- DOI: 10.1097/QAI.0000000000002707
HIV-1 Recent Infection Testing Algorithm With Antiretroviral Drug Detection to Improve Accuracy of Incidence Estimates
Abstract
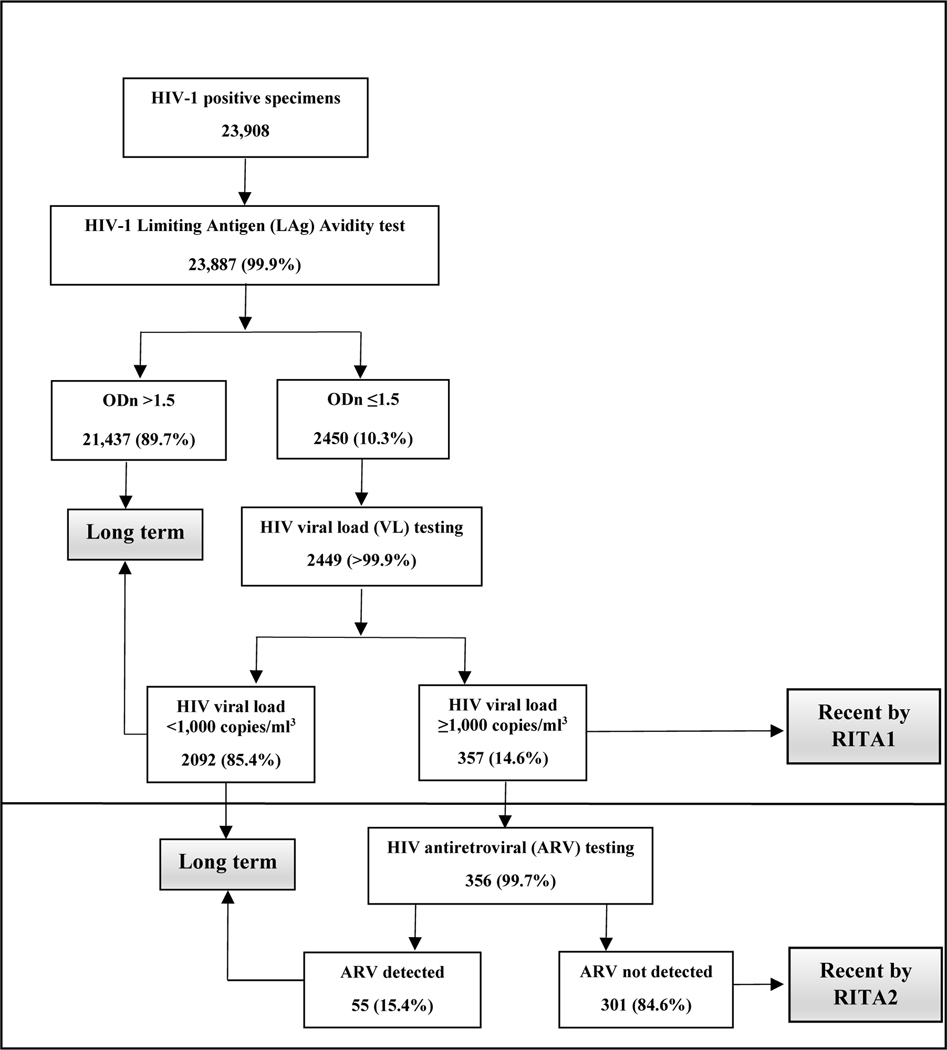
Background: HIV-1 incidence calculation currently includes recency classification by HIV-1 incidence assay and unsuppressed viral load (VL ≥ 1000 copies/mL) in a recent infection testing algorithm (RITA). However, persons with recent classification not virally suppressed and taking antiretroviral (ARV) medication may be misclassified.
Setting: We used data from 13 African household surveys to describe the impact of an ARV-adjusted RITA on HIV-1 incidence estimates.
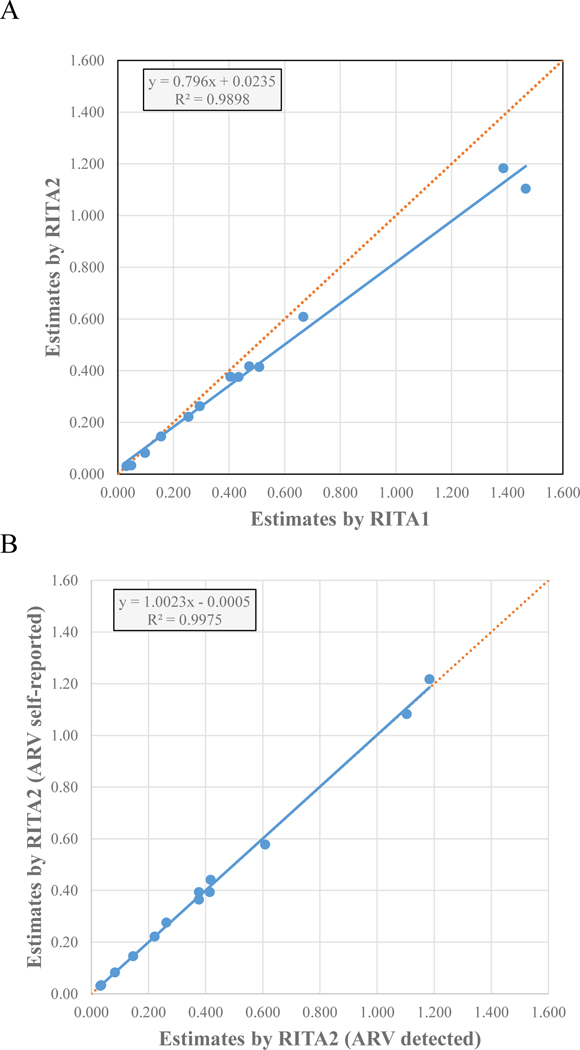
Methods: HIV-seropositive samples were tested for recency using the HIV-1 Limiting Antigen (LAg)-Avidity enzyme immunoassay, HIV-1 viral load, ARVs used in each country, and ARV drug resistance. LAg-recent result was defined as normalized optical density values ≤1.5. We compared HIV-1 incidence estimates using 2 RITA: RITA1: LAg-recent + VL ≥ 1000 copies/mL and RITA2: RITA1 + undetectable ARV. We explored RITA2 with self-reported ARV use and with clinical history.
Results: Overall, 357 adult HIV-positive participants were classified as having recent infection with RITA1. RITA2 reclassified 55 (15.4%) persons with detectable ARV as having long-term infection. Those with detectable ARV were significantly more likely to be aware of their HIV-positive status (84% vs. 10%) and had higher levels of drug resistance (74% vs. 26%) than those without detectable ARV. RITA2 incidence was lower than RITA1 incidence (range, 0%-30% decrease), resulting in decreased estimated new infections from 390,000 to 341,000 across the 13 countries. Incidence estimates were similar using detectable or self-reported ARV (R2 > 0.995).
Conclusions: Including ARV in RITA2 improved the accuracy of HIV-1 incidence estimates by removing participants with likely long-term HIV infection.
Copyright © 2021 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
As an inventor of LAg-Avidity EIA, B.S.P. receives royalties from the sale of test kits sold by the manufacturer per US government policy. The other authors have no conflicts of interest to disclose.
Figures
References
-
- 90–90-90 An ambitious treatment target to help end the AIDS epidemic. 2014. 2020, at https://files.unaids.org/en/media/unaids/contentassets/documents/unaidsp....)
-
- Justman JE, Mugurungi O, El-Sadr WM. HIV Population Surveys - Bringing Precision to the Global Response. The New England journal of medicine 2018;378:1859–61. - PubMed
-
- Nkambule RN-BH, Mnisi Z, Ao TT, Ginindza C, Duong YT, Patel H, Saito S, Philip NM, Brown K, Draghi C, Voetsch AC, Mabuza K, Zwane A, Sahabo R, Okello V, Dobbs T, Parekh B, Ryan C, Justman J. Substantial progress in confronting the HIV epidemic in Swaziland: first evidence of national impact. 9th IAS Conference on HIV Science 2017; Paris, France. p. 564.
-
- Monitoring HIV Impact Using Population-based Surveys. 2015. at https://www.unaids.org/sites/default/files/media_asset/JC2763_Population....)
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
