

Hospital-treated infectious diseases and the risk of dementia: a large, multicohort, observational study with a replication cohort
- PMID: 34166620
- PMCID: PMC8592915
- DOI: 10.1016/S1473-3099(21)00144-4
Hospital-treated infectious diseases and the risk of dementia: a large, multicohort, observational study with a replication cohort
Abstract
Background: Infections have been hypothesised to increase the risk of dementia. Existing studies have included a narrow range of infectious diseases, relied on short follow-up periods, and provided little evidence for whether the increased risk is limited to specific dementia subtypes or attributable to specific microbes rather than infection burden. We aimed to compare the risk of Alzheimer's disease and other dementias across a wide range of hospital-treated bacterial and viral infections in two large cohorts with long follow-up periods.
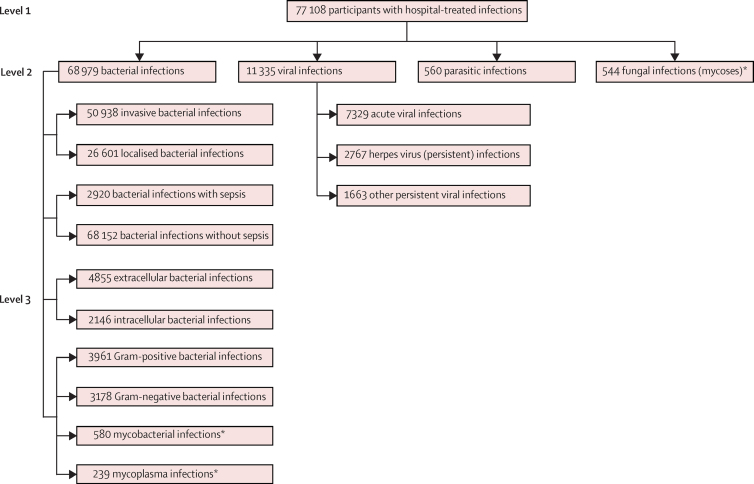
Methods: In this large, multicohort, observational study, the analysis was based on a primary cohort consisting of pooled individual-level data from three prospective cohort studies in Finland (the Finnish Public Sector study, the Health and Social Support study, and the Still Working study) and an independent replication cohort from the UK Biobank. Community-dwelling adults (≥18 years) with no dementia at study entry were included. Follow-up was until Dec 31, 2012, in the Health and Social Support study, Dec 31, 2016, in the public sector study and the Still Working study, and Feb 7, 2018, in the replication cohort. Through record linkage to national hospital inpatient registers, we ascertained exposure to 925 infectious diseases (using the International Classification of Diseases 10th Revision codes) before dementia onset, and identified incident dementia from hospital records, medication reimbursement entitlements, and death certificates. Hazard ratios (HRs) for the associations of each infectious disease or disease group (index infection) with incident dementia were assessed by use of Cox proportional hazards models. We then repeated the analysis after excluding incident dementia cases that occurred during the first 10 years after initial hospitalisation due to the index infection.
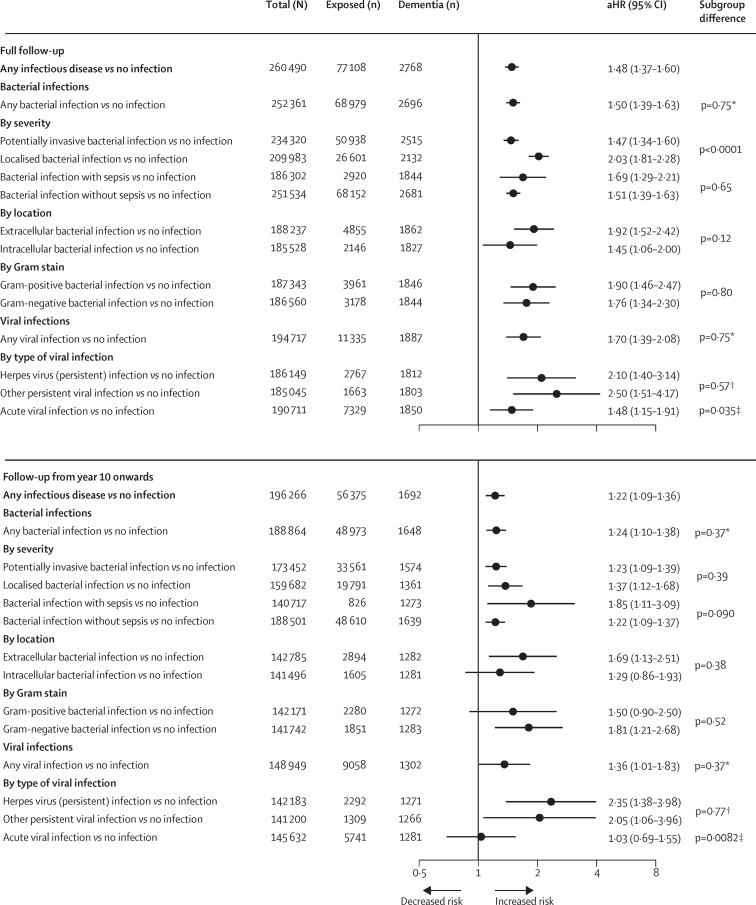
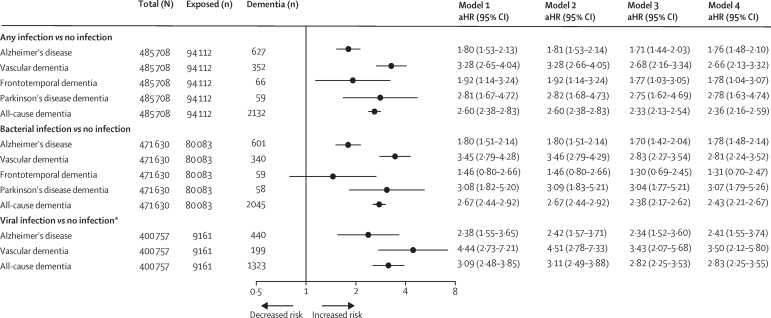
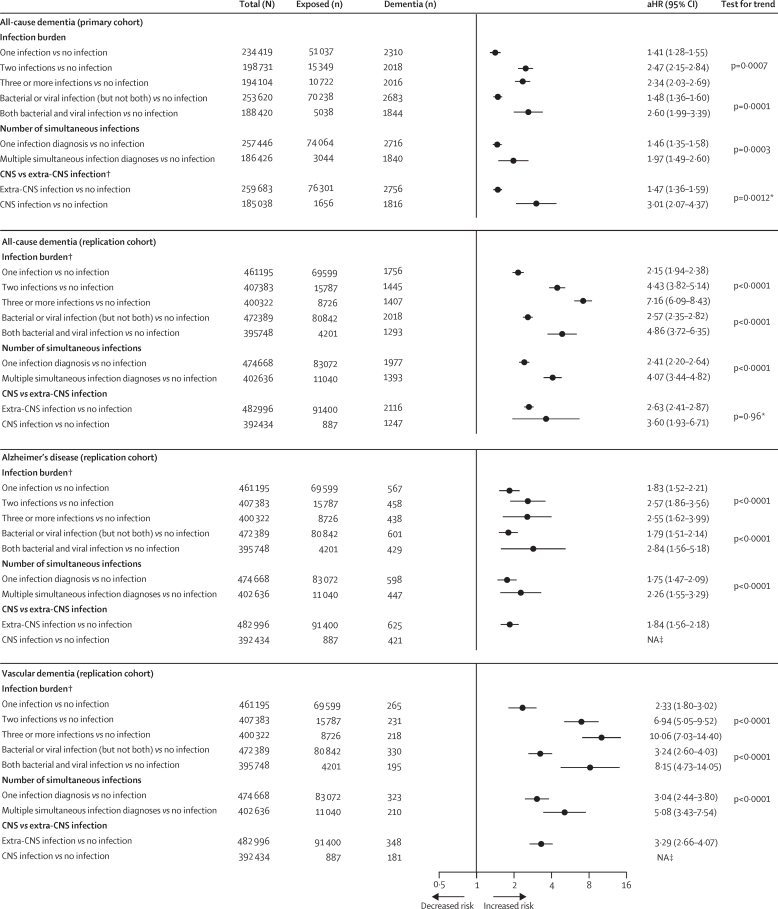
Findings: From March 1, 1986, to Jan 1, 2005, 260 490 people were included in the primary cohort, and from Dec 19, 2006, to Oct 1, 2010, 485 708 people were included in the replication cohort. In the primary cohort analysis based on 3 947 046 person-years at risk (median follow-up 15·4 years [IQR 9·8-21·0]), 77 108 participants had at least one hospital-treated infection before dementia onset and 2768 developed dementia. Hospitalisation for any infectious disease was associated with increased dementia risk in the primary cohort (adjusted HR [aHR] 1·48 [95% CI 1·37-1·60]) and replication cohort (2·60 [2·38-2·83]). The association remained when analyses were restricted to new dementia cases that occurred more than 10 years after infection (aHR 1·22 [95% CI 1·09-1·36] in the primary cohort, the replication cohort had insufficient follow-up data for this analysis), and when comorbidities and other dementia risk factors were considered. There was evidence of a dose-response association between the number of episodes of hospital-treated infections and dementia risk in both cohorts (ptrend=0·0007). Although the greatest dementia risk was seen for central nervous system (CNS) infections versus no infection (aHR 3·01 [95% CI 2·07-4·37]), excess risk was also evident for extra-CNS infections (1·47 [1·36-1·59]). Although we found little difference in the infection-dementia association by type of infection, associations were stronger for vascular dementia than for Alzheimer's disease (aHR 2·09 [95% CI 1·59-2·75] versus aHR 1·20 [1·08-1·33] in the primary cohort and aHR 3·28 [2·65-4·04] versus aHR 1·80 [1·53-2·13] in the replication cohort).
Interpretation: Severe infections requiring hospital treatment are associated with long-term increased risk of dementia, including vascular dementia and Alzheimer's disease. This association is not limited to CNS infections, suggesting that systemic effects are sufficient to affect the brain. The absence of infection specificity combined with evidence of dose-response relationships between infectious disease burden and dementia risk support the hypothesis that increased dementia risk is driven by general inflammation rather than specific microbes.
Funding: UK Medical Research Council, US National Institute on Aging, Wellcome Trust, NordForsk, Academy of Finland, and Helsinki Institute of Life Science.
Copyright © 2021 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests PNS reports funding from the Helsinki Institute of Life Science, NordForsk, and the Academy of Finland during the conduct of the study, and from the Finnish Foundation for Alcohol Studies outside of the submitted work. JVL reports funding from the Academy of Finland during the conduct of the study. STN reports funding from NordForsk during the conduct of the study. TES reports funding from the Academy of Finland; consultation fees from Servier, Orion, and Novartis outside the submitted work; and is a member of the European Geriatric Medicine Society special interest group on Cardiovascular Medicine in Older People and Diabetes in older people. MK reports funding from the Helsinki Institute of Life Science, the Academy of Finland, NordForsk, UK Medical Research Council, the US National Institute on Aging, and the Wellcome Trust during the conduct of the study. CH, JV, and ME report funding from the Academy of Finland. All other authors declare no competing interests.
Figures
Comment in
-
Should infectious diseases be targeted to prevent dementias?Lancet Infect Dis. 2021 Nov;21(11):1477-1478. doi: 10.1016/S1473-3099(21)00258-9. Epub 2021 Jun 21. Lancet Infect Dis. 2021. PMID: 34166619 No abstract available.
References
-
- Itzhaki RF, Golde TE, Heneka MT, Readhead B. Do infections have a role in the pathogenesis of Alzheimer disease? Nat Rev Neurol. 2020;16:193–197. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
