

Cardiac Troponin Thresholds and Kinetics to Differentiate Myocardial Injury and Myocardial Infarction
- PMID: 34167318
- PMCID: PMC8360674
- DOI: 10.1161/CIRCULATIONAHA.121.054302
Cardiac Troponin Thresholds and Kinetics to Differentiate Myocardial Injury and Myocardial Infarction
Abstract
Background: Although the 99th percentile is the recommended diagnostic threshold for myocardial infarction, some guidelines also advocate the use of higher troponin thresholds to rule in myocardial infarction at presentation. It is unclear whether the magnitude or change in troponin concentration can differentiate causes of myocardial injury and infarction in practice.
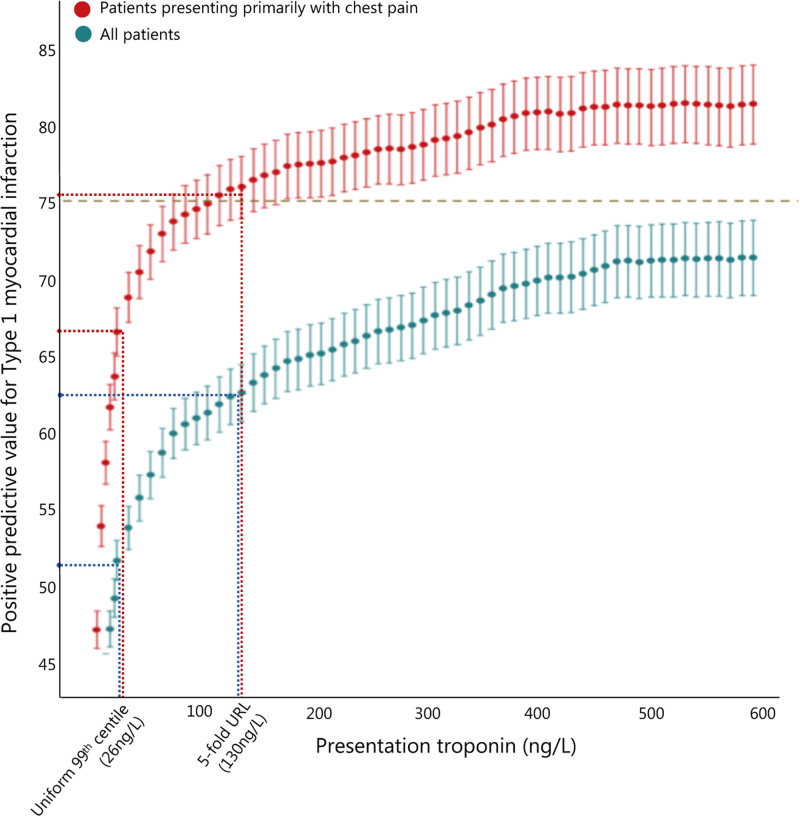
Methods: In a secondary analysis of a multicenter randomized controlled trial, we identified 46 092 consecutive patients presenting with suspected acute coronary syndrome without ST-segment-elevation myocardial infarction. High-sensitivity cardiac troponin I concentrations at presentation and on serial testing were compared between patients with myocardial injury and infarction. The positive predictive value and specificity were determined at the sex-specific 99th percentile upper reference limit and rule-in thresholds of 64 ng/L and 5-fold of the upper reference limit for a diagnosis of type 1 myocardial infarction.
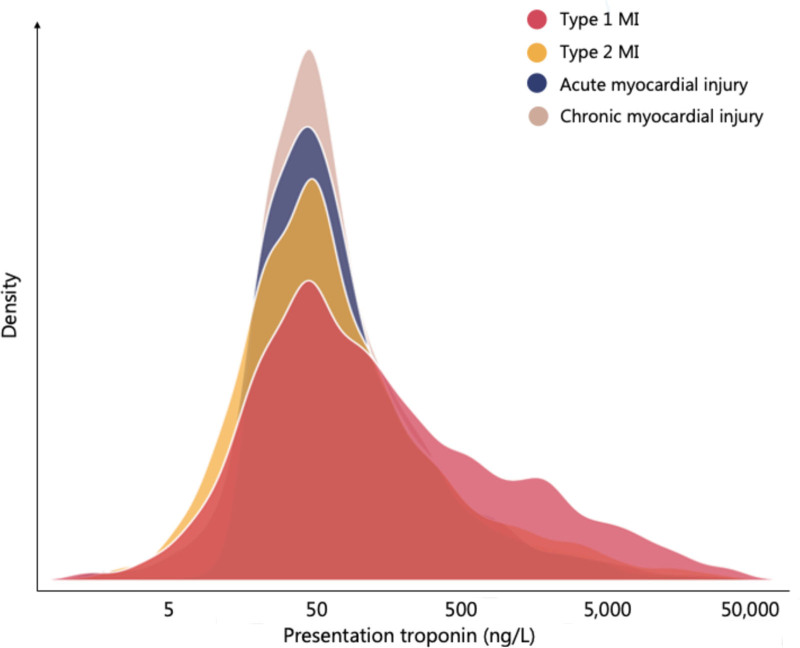
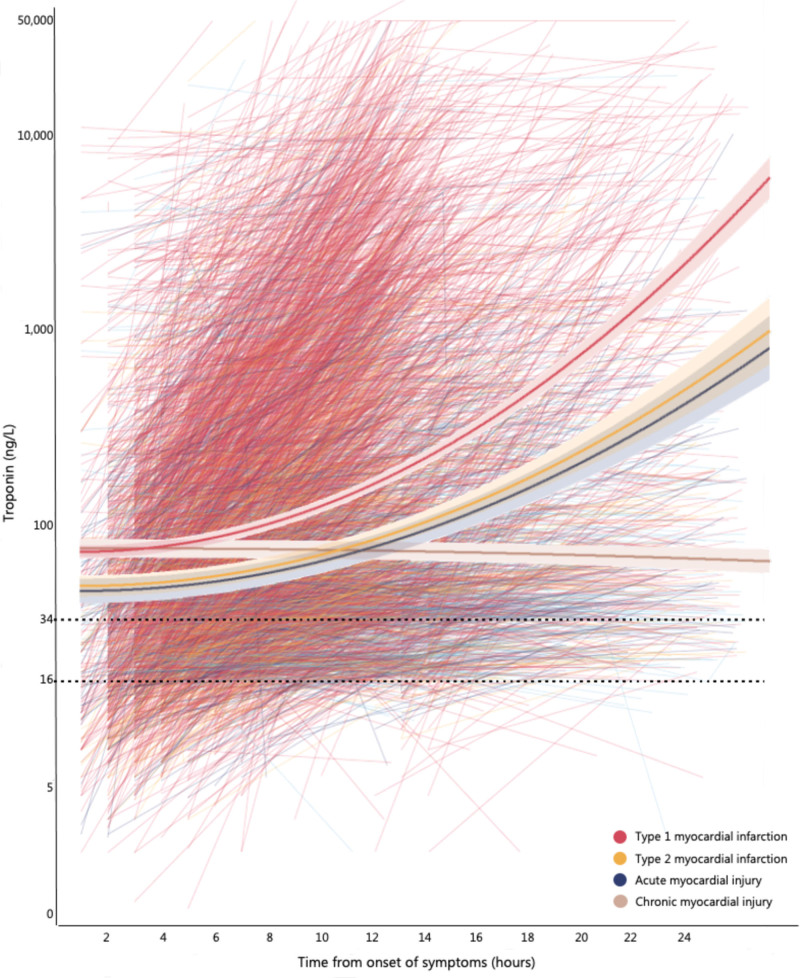
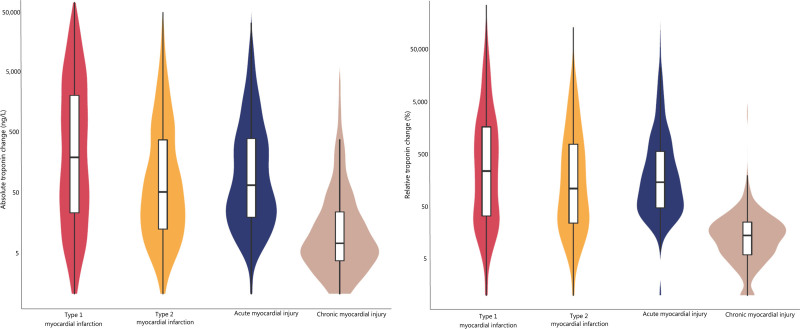
Results: Troponin was above the 99th percentile in 8188 patients (18%). The diagnosis was type 1 or type 2 myocardial infarction in 50% and 14% and acute or chronic myocardial injury in 20% and 16%, respectively. Troponin concentrations were similar at presentation in type 1 (median [25th-75th percentile] 91 [30-493] ng/L) and type 2 (50 [22-147] ng/L) myocardial infarction and in acute (50 [26-134] ng/L) and chronic (51 [31-130] ng/L) myocardial injury. The 99th percentile and rule-in thresholds of 64 ng/L and 5-fold upper reference limit gave a positive predictive value of 57% (95% CI, 56%-58%), 59% (58%-61%), and 62% (60%-64%) and a specificity of 96% (96%-96%), 96% (96%-96%), and 98% (97%-98%), respectively. The absolute, relative, and rate of change in troponin concentration were highest in patients with type 1 myocardial infarction (P<0.001 for all). Discrimination improved when troponin concentration and change in troponin were combined compared with troponin concentration at presentation alone (area under the curve, 0.661 [0.642-0.680] versus 0.613 [0.594-0.633]).
Conclusions: Although we observed important differences in the kinetics, cardiac troponin concentrations at presentation are insufficient to distinguish type 1 myocardial infarction from other causes of myocardial injury or infarction in practice and should not guide management decisions in isolation. Registration: URL: https://www.clinicaltrials.gov; Unique identifier: NCT01852123.
Keywords: kinetics; myocardial infarction; predictive value of tests; troponin.
Figures
References
-
- Thygesen K, Alpert JS, Jaffe AS, Chaitman BR, Bax JJ, Morrow DA, White HD. Fourth universal definition of myocardial infarction (2018). Eur Heart J. 2019;40:237–269. doi: 10.1016/j.jacc.2018.08.1038 - PubMed
-
- Chapman AR, Adamson PD, Shah ASV, Anand A, Strachan FE, Ferry AV, Lee KK, Berry C, Findlay I, Cruikshank A, et al. ; High-STEACS Investigators. High-sensitivity cardiac troponin and the universal definition of myocardial infarction. Circulation. 2020;141:161–171. doi: 10.1161/CIRCULATIONAHA.119.042960 - PMC - PubMed
-
- Shah ASV, Sandoval Y, Noaman A, Sexter A, Vaswani A, Smith SW, Gibbins M, Griffiths M, Chapman AR, Strachan FE, et al. . Patient selection for high sensitivity cardiac troponin testing and diagnosis of myocardial infarction: prospective cohort study. BMJ. 2017;359:j4788. doi: 10.1136/bmj.j4788 - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
