

Healthcare needs, expectations, utilization, and experienced treatment effects in patients with hereditary spastic paraplegia: a web-based survey in the Netherlands
- PMID: 34167574
- PMCID: PMC8223283
- DOI: 10.1186/s13023-021-01915-0
Healthcare needs, expectations, utilization, and experienced treatment effects in patients with hereditary spastic paraplegia: a web-based survey in the Netherlands
Abstract
Background: We aimed to identify healthcare needs, expectations, utilization, and the experienced treatment effects in a population of Dutch patients with hereditary spastic paraplegia (HSP).
Methods: We distributed an online questionnaire among 194 adult persons with HSP in the Netherlands, of which 166 returned a fully completed version. After applying predefined exclusion criteria, 109 questionnaires from persons with pure HSP were analysed.
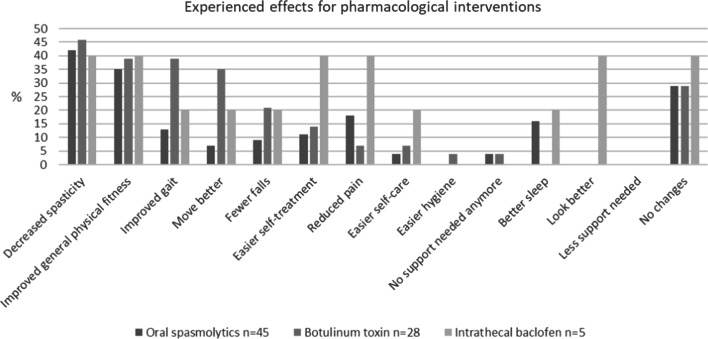
Results: Healthcare needs and expectations were primarily focused on the relief of muscle stiffness and reduction of balance and gait impairments (65-80%), but many participants also expressed needs regarding relief of non-motor symptoms (e.g. pain, fatigue), emotional problems, impaired sleep and self-care capacity, and participation problems (> 60%). Remarkably, despite these frequent needs, relatively few participants (< 33%) expected to be able to improve in these additional domains. Rehabilitation physicians and physiotherapists were more frequently consulted than neurologists and occupational therapists, respectively. Physiotherapy was the most often proposed non-pharmacological intervention (85%), followed by orthopedic footwear (55%) and splints (28%). Approximately one third of the participants was never offered any pharmacological (spasmolytic) treatment. Spasmolytic oral drugs, injections, and intrathecal baclofen were given to 41%, 26%, and 5% of the participants, respectively. Independent of the type of pharmacological intervention, 35-46% of these participants experienced decreased spastiticy and improved general fitness. Other experienced effects differed per type of intervention.
Conclusions: Based on this web-based survey in the Netherlands, there seems to be ample room for improvement to meet and attune the healthcare needs and expectations of people with HSP concerning both their motor and non-motor symptoms and functional limitations. In addition, the provision of adequate information about non-pharmacological and pharmacological interventions seems to be insufficient for many patients to allow shared decision making. These conclusions warrant a more pro-active attitude of healthcare providers as well as an interdisciplinary approach for a substantial proportion of the HSP population, also involving professionals with a primary occupational and/or psychosocial orientation.
Keywords: Experienced treatment effects; Healthcare utilization; Hereditary spastic paraplegia; Needs assessment; Patient-reported outcomes; Spasticity; Survey.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- van Lith BJH, Kerstens HCJW, van den Bemd LAC, der Sanden MWGN, Weerdesteyn V, Smeets RJEM, et al. Experienced complaints, activity limitations and loss of motor capacities in patients with pure hereditary spastic paraplegia: a web-based survey in the Netherlands. Orphanet J Rare Dis. 2020;15(1):64020–1338-4. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
