

Neuroimaging Findings in Retinal Vasculopathy with Cerebral Leukoencephalopathy and Systemic Manifestations
- PMID: 34167956
- PMCID: PMC8423035
- DOI: 10.3174/ajnr.A7194
Neuroimaging Findings in Retinal Vasculopathy with Cerebral Leukoencephalopathy and Systemic Manifestations
Abstract
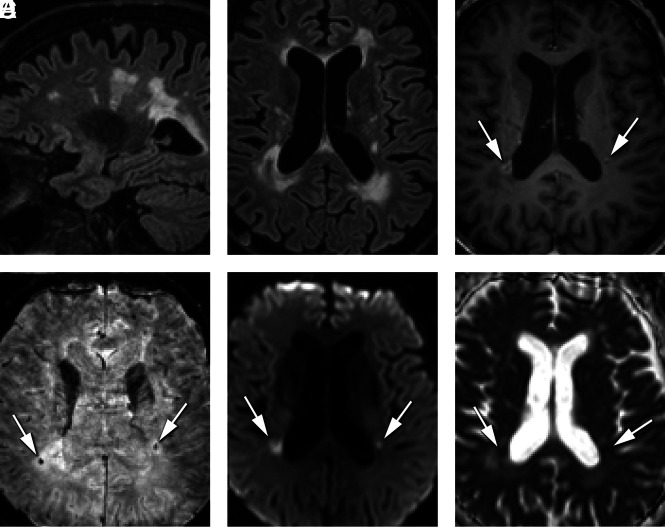
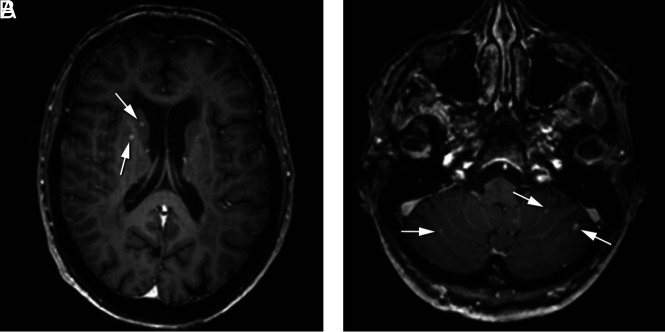
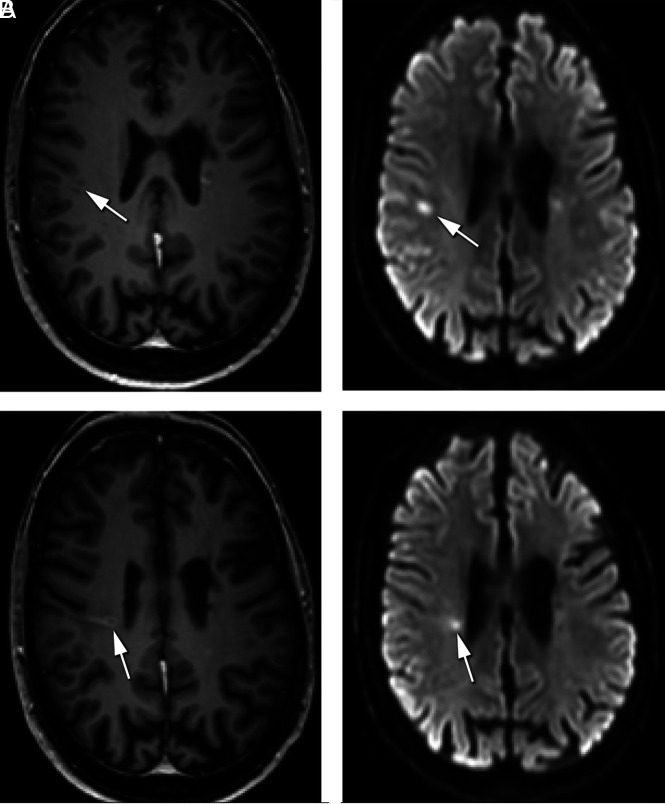
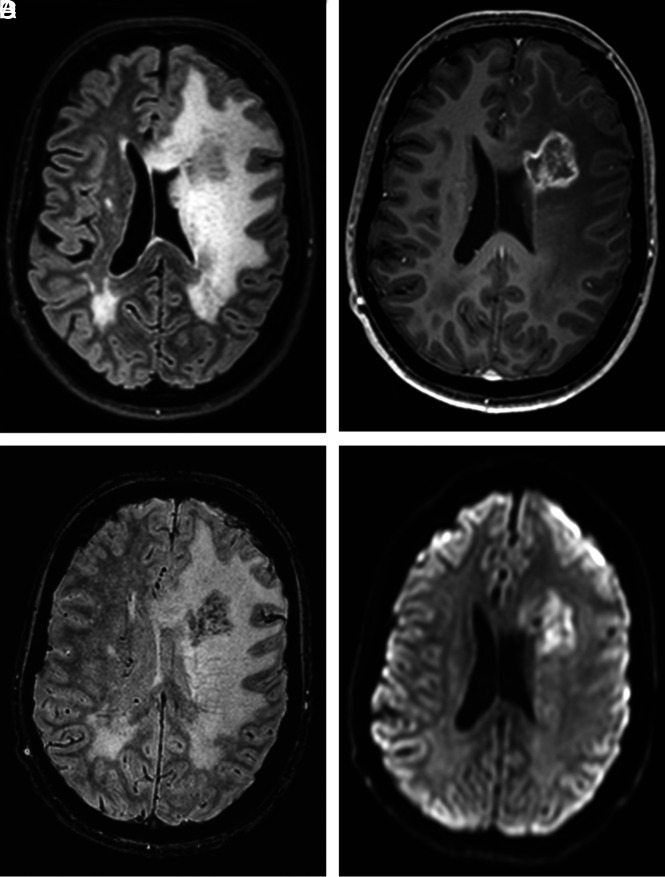
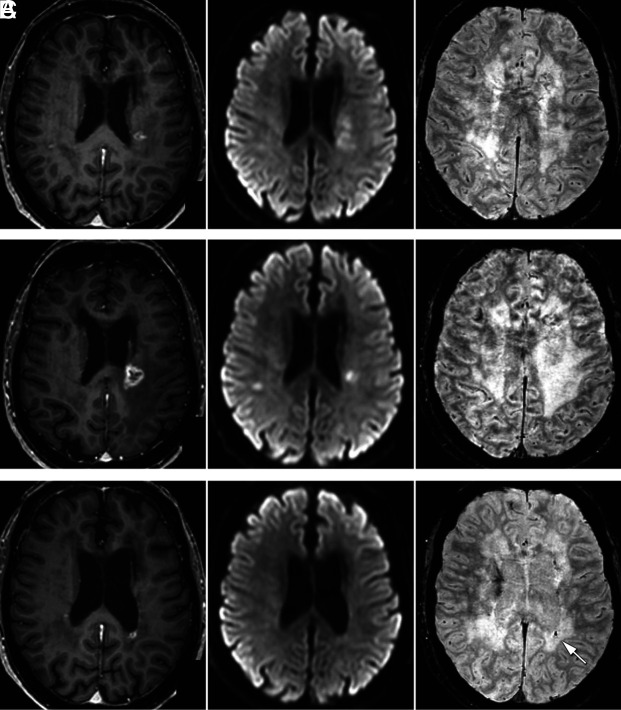
Retinal vasculopathy with cerebral leukoencephalopathy and systemic manifestations is caused by TREX1 mutations. High-quality systematic follow-up neuroimaging findings have not been described in presymptomatic and symptomatic mutation carriers. We present MR imaging findings of 29 TREX1 mutation carriers (20-65 years of age) and follow-up of 17 mutation carriers (30-65 years of age). Mutation carriers younger than 40 years of age showed a notable number of punctate white matter lesions, but scan findings were generally unremarkable. From 40 years of age onward, supratentorial lesions developed with long-term contrast enhancement (median, 24 months) and diffusion restriction (median, 8 months). In these lesions, central susceptibility artifacts developed, at least partly corresponding to calcifications on available CT scans. Some lesions (n = 2) additionally showed surrounding edema and mass effect (pseudotumors). Cerebellar punctate enhancing lesions developed mainly in individuals older than 50 years of age. These typical neuroimaging findings should aid neuroradiologic recognition of retinal vasculopathy with cerebral leukoencephalopathy and systemic manifestations, which may enable early treatment of manifestations of the disease.
© 2021 by American Journal of Neuroradiology.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical