

Intracerebral administration of CTLA-4 and PD-1 immune checkpoint blocking monoclonal antibodies in patients with recurrent glioblastoma: a phase I clinical trial
- PMID: 34168003
- PMCID: PMC8231061
- DOI: 10.1136/jitc-2020-002296
Intracerebral administration of CTLA-4 and PD-1 immune checkpoint blocking monoclonal antibodies in patients with recurrent glioblastoma: a phase I clinical trial
Abstract
Background: Patients with recurrent glioblastoma (rGB) have a poor prognosis with a median overall survival (OS) of 30-39 weeks in prospective clinical trials. Intravenous administration of programmed cell death protein 1 and cytotoxic T-lymphocyte-associated antigen 4 inhibitors has low activity in patients with rGB. In this phase I clinical trial, intracerebral (IC) administration of ipilimumab (IPI) and nivolumab (NIVO) in combination with intravenous administration of NIVO was investigated.
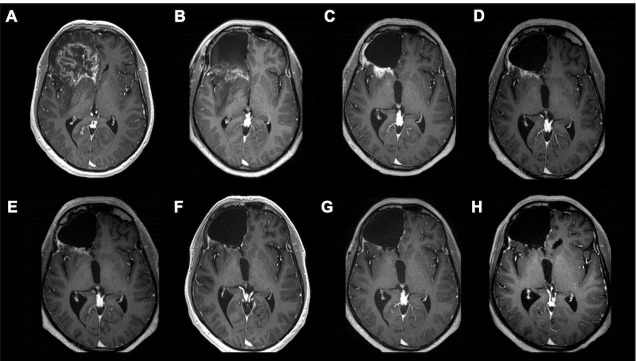
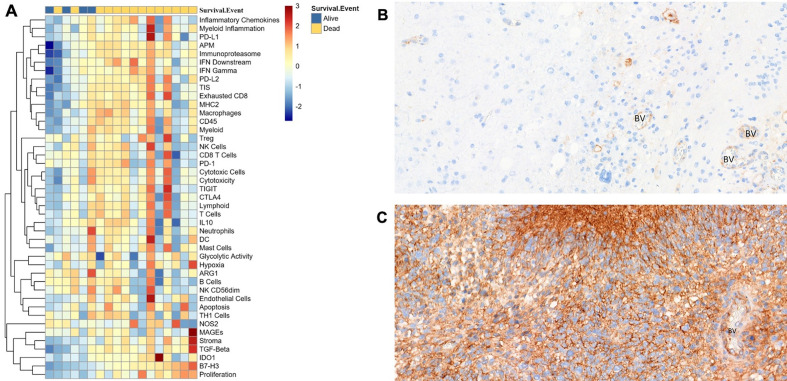
Methods: Within 24 hours following the intravenous administration of a fixed dose (10 mg) of NIVO, patients underwent a maximal safe resection, followed by injection of IPI (10 mg; cohort-1), or IPI (5 mg) plus NIVO (10 mg; cohort-2) in the brain tissue lining the resection cavity. Intravenous administration of NIVO (10 mg) was repeated every 2 weeks (max. five administrations). Next generation sequencing and RNA gene expression profiling was performed on resected tumor tissue.
Results: Twenty-seven patients were enrolled (cohort-1: n=3; cohort-2: n=24). All patients underwent maximal safe resection and planned IC administrations and preoperative NIVO. Thirteen patients (cohort-1: n=3; cohort-2: n=10) received all five postoperative intravenous doses of NIVO. In cohort-2, 14 patients received a median of 3 (range 1-4) intravenous doses. Subacute postoperative neurological deterioration (n=2) was reversible on steroid treatment; no other central nervous system toxicity was observed. Immune-related adverse events were infrequent and mild. GB recurrence was diagnosed in 26 patients (median progression-free survival (PFS) is 11.7 weeks (range 2-152)); 21 patients have died due to progression. Median OS is 38 weeks (95% CI: 27 to 49) with a 6-month, 1-year, and 2-year OS-rate of, respectively, 74.1% (95% CI: 57 to 90), 40.7% (95% CI: 22 to 59), and 27% (95% CI: 9 to 44). OS compares favorable against a historical cohort (descriptive Log-Rank p>0.003). No significant difference was found with respect to PFS (descriptive Log-Rank test p>0.05). A higher tumor mRNA expression level of B7-H3 was associated with a significantly worse survival (multivariate Cox logistic regression, p>0.029).
Conclusion: IC administration of NIVO and IPI following maximal safe resection of rGB was feasible, safe, and associated with encouraging OS.
Trial registration: NCT03233152.
Keywords: brain neoplasms; immunotherapy.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: Julia Katharina Schwarze reports non-financial support from MSD and Amgen; grants for research from Kom op tegen Kanker, Stichting tegen Kanker. Gil Awada reports grants and nonfinancial support from Pfizer, Novartis; non-financial support from MSD, Astellas; personal fees from Novartis; grants from Kom op tegen Kanker, Stichting tegen Kanker. Bart Neyns reports personal financial compensation from Roche, Bristol-Myers Squibb, Merck Sharp & Dohme, Novartis, AstraZeneca for public speaking, consultancy and participation in advisory board meeting. The institution (UZ Brussel) received research funding related to research projects conducted by Bart Neyns from Pfizer, Novartis, Roche, Merck-Serono. The other authors do not declare any competing interests.
Figures



References
-
- Stupp R, Hegi ME, Mason WP, et al. . Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol 2009;10:459–66. 10.1016/S1470-2045(09)70025-7 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials