

Rheumatoid arthritis-interstitial lung disease: manifestations and current concepts in pathogenesis and management
- PMID: 34168062
- PMCID: PMC9489133
- DOI: 10.1183/16000617.0011-2021
Rheumatoid arthritis-interstitial lung disease: manifestations and current concepts in pathogenesis and management
Abstract
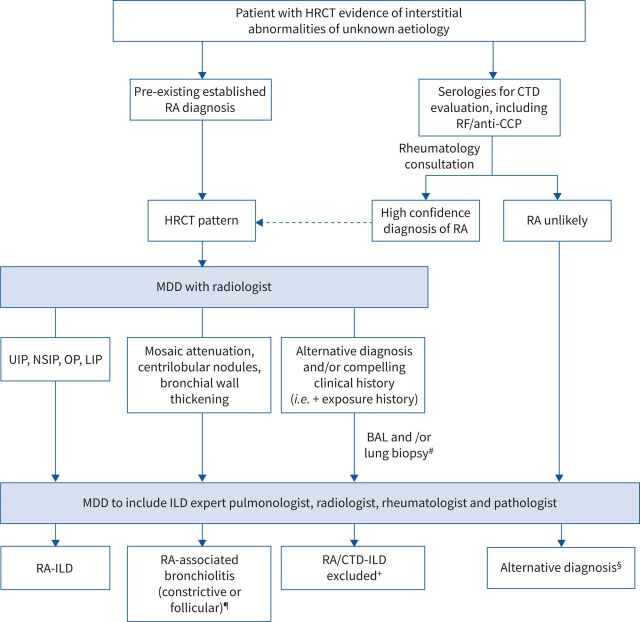
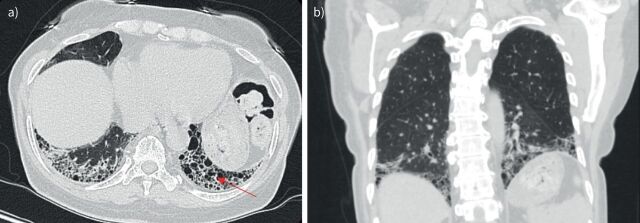
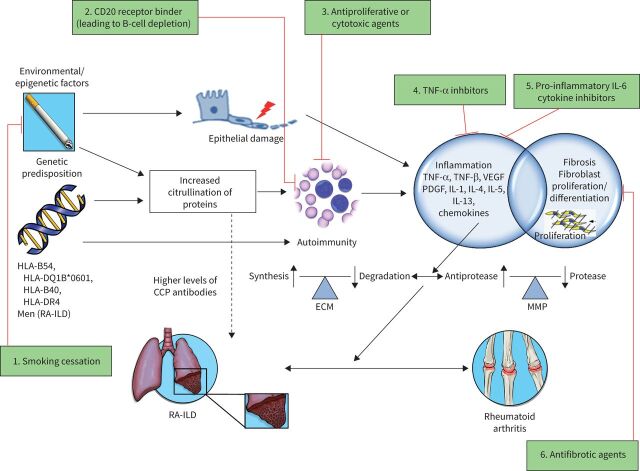
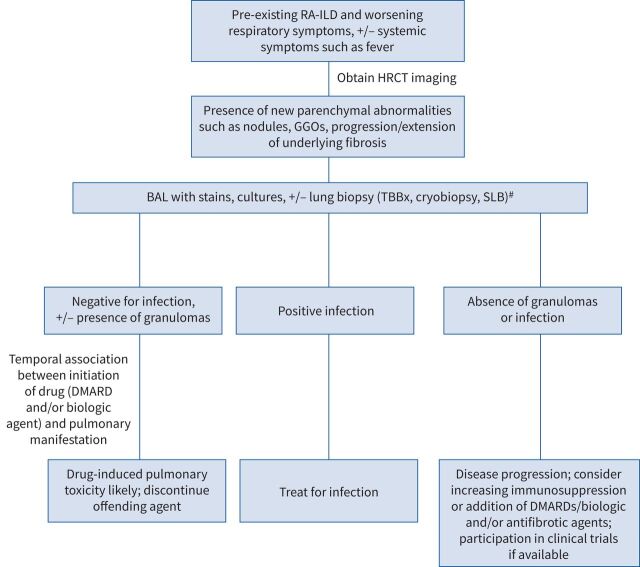
Rheumatoid arthritis (RA) is a systemic inflammatory disorder, with the most common extra-articular manifestation of RA being lung involvement. While essentially any of the lung compartments can be affected and manifest as interstitial lung disease (ILD), pleural effusion, cricoarytenoiditis, constrictive or follicular bronchiolitis, bronchiectasis, pulmonary vasculitis, and pulmonary hypertension, RA-ILD is a leading cause of death in patients with RA and is associated with significant morbidity and mortality. In this review, we focus on the common pulmonary manifestations of RA, RA-ILD and airway disease, and discuss evolving concepts in the pathogenesis of RA-associated pulmonary fibrosis, as well as therapeutic strategies, and have revised our previous review on the topic. A rational clinical approach for the diagnosis and management of RA-ILD, as well as an approach to patients with clinical worsening in the setting of treatment with disease-modifying agents, is included. Future directions for research and areas of unmet need in the realm of RA-associated lung disease are raised.
Copyright ©The authors 2021.
Conflict of interest statement
Conflict of interest: S. Kadura has nothing to disclose. Conflict of interest: G. Raghu reports personal fees and other funding from Boehringer-Ingelheim and other funding from Roche-Genentech, outside the submitted work.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical