

CD27-CD38lowCD21low B-Cells Are Increased in Axial Spondyloarthritis
- PMID: 34168654
- PMCID: PMC8217653
- DOI: 10.3389/fimmu.2021.686273
CD27-CD38lowCD21low B-Cells Are Increased in Axial Spondyloarthritis
Abstract
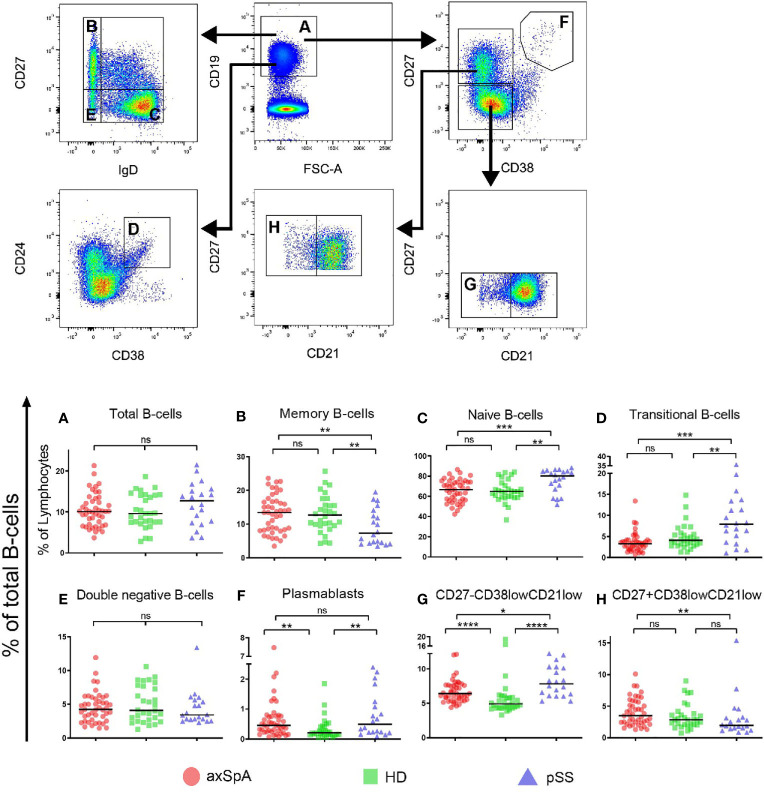
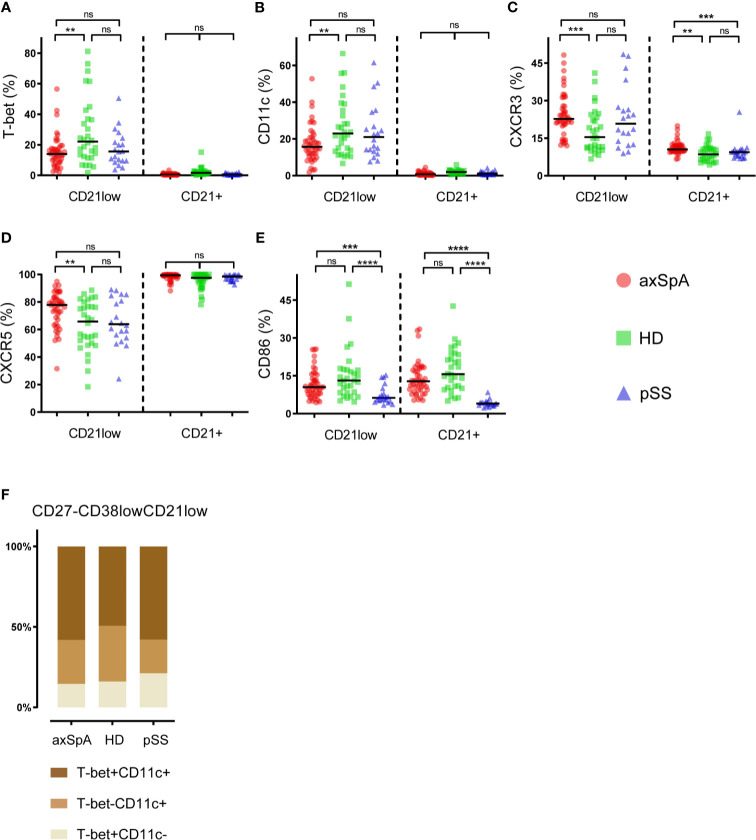
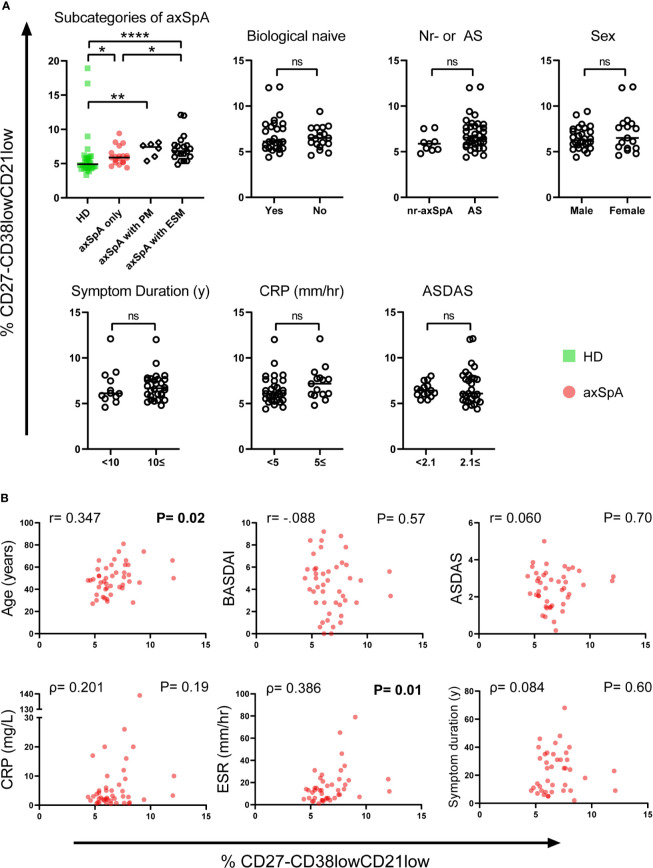
B-cells have received little attention in axial spondyloarthritis (axSpA) and for this reason their role in pathogenesis remains unclear. However, there are indications that B-cells may be involved in the disease process. Our objective was to obtain insights into the composition of the peripheral B-cell compartment of axSpA patients compared to healthy donors (HD) and patients with primary Sjögren's syndrome (pSS), a typical B-cell-associated autoimmune disease. Special emphasis was given to CD27-negative B-cells expressing low levels of CD21 (CD21low B-cells), since this subset is implicated in autoimmune diseases with strong involvement of B-cells. Transitional B-cells (CD38hi) were excluded from the analysis of the CD27-CD21low B-cell compartment. This study included 45 axSpA patients, 20 pSS patients and 30 HDs. Intriguingly, compared to HDs the frequency of CD27-CD38lowCD21low B-cells was significantly elevated in both axSpA and pSS patients (P<0.0001 for both comparisons). The frequency of CD27-CD38lowCD21low B-cells expressing the activation-induced immune markers T-bet and CD11c was decreased in axSpA patients compared to HDs. A higher proportion of CD27-CD38lowCD21low B-cells expressed the chemokine receptor CXCR3 in axSpA compared to HDs, suggestive for active involvement of these cells in an inflammatory process. The frequency of CD27-CD38lowCD21low B-cells in axSpA patients correlated positively with age and erythrocyte sedimentation rate. Furthermore, axSpA patients with extra-skeletal manifestations (ESM) showed increased frequencies of CD27-CD38lowCD21low B-cells compared to patients without ESM. In conclusion, our findings are suggestive of active B-cell involvement in the pathogenesis of axSpA, against prevailing dogma.
Keywords: B-cells; CD21low B-cells; Sjögren’s syndrome; ankylosing spondylitis; autoimmunity; axial spondyloarthritis.
Copyright © 2021 Wilbrink, Spoorenberg, Arends, van der Geest, Brouwer, Bootsma, Kroese and Verstappen.
Conflict of interest statement
AS has received grant/research support from Abbvie, Pfizer, Union Chimique Belge (UCB), Novartis and acted as a consultant for Abbvie, Pfizer, MSD, UCB, Lilly and Novartis. SA has received grant/research support from Pfizer. KG has received a speaker fee from Roche. EB has received consultancy and speaker fees from Roche. HB has received unrestricted grants from Bristol Myers Squibb (BMS) and Roche, consultant for BMS, Roche, Novartis, MedImmune, UCB, speaker for BMS and Novartis. FK has received unrestricted grants from BMS, is consultant for BMS, speaker for BMS Roche and Jannsen-Cilag. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
B Cell Receptor Repertoire Analysis of the CD21lo B Cell Compartment in Healthy Individuals, Patients With Sjögren's Disease, and Patients With Radiographic Axial Spondyloarthritis.Eur J Immunol. 2025 Feb;55(2):e202451398. doi: 10.1002/eji.202451398. Epub 2024 Dec 20. Eur J Immunol. 2025. PMID: 39707660 Free PMC article.
-
Deep Phenotyping of CD11c+ B Cells in Systemic Autoimmunity and Controls.Front Immunol. 2021 Mar 12;12:635615. doi: 10.3389/fimmu.2021.635615. eCollection 2021. Front Immunol. 2021. PMID: 33777025 Free PMC article.
-
Peripheral regulatory cells immunophenotyping in primary Sjögren's syndrome: a cross-sectional study.Arthritis Res Ther. 2013;15(3):R68. doi: 10.1186/ar4245. Arthritis Res Ther. 2013. PMID: 23800367 Free PMC article.
-
B cells in Sjögren's syndrome: indications for disturbed selection and differentiation in ectopic lymphoid tissue.Arthritis Res Ther. 2007;9(4):218. doi: 10.1186/ar2210. Arthritis Res Ther. 2007. PMID: 17697366 Free PMC article. Review.
-
The meaning of anti-Ro and anti-La antibodies in primary Sjögren's syndrome.Autoimmun Rev. 2011 Jan;10(3):123-5. doi: 10.1016/j.autrev.2010.09.001. Epub 2010 Sep 15. Autoimmun Rev. 2011. PMID: 20833272 Review.
Cited by
-
Age-associated B cells in autoimmune diseases.Cell Mol Life Sci. 2022 Jul 7;79(8):402. doi: 10.1007/s00018-022-04433-9. Cell Mol Life Sci. 2022. PMID: 35798993 Free PMC article. Review.
-
Aberrant B cell receptor signaling responses in circulating double-negative 2 B cells from radiographic axial spondyloarthritis patients.J Transl Autoimmun. 2025 Jan 23;10:100270. doi: 10.1016/j.jtauto.2025.100270. eCollection 2025 Jun. J Transl Autoimmun. 2025. PMID: 39974741 Free PMC article.
-
B Cell Receptor Repertoire Analysis of the CD21lo B Cell Compartment in Healthy Individuals, Patients With Sjögren's Disease, and Patients With Radiographic Axial Spondyloarthritis.Eur J Immunol. 2025 Feb;55(2):e202451398. doi: 10.1002/eji.202451398. Epub 2024 Dec 20. Eur J Immunol. 2025. PMID: 39707660 Free PMC article.
-
A close-up on the expanding landscape of CD21-/low B cells in humans.Clin Exp Immunol. 2022 Dec 31;210(3):217-229. doi: 10.1093/cei/uxac103. Clin Exp Immunol. 2022. PMID: 36380692 Free PMC article. Review.
-
Emerging biochemical, microbial and immunological evidence in the search for why HLA-B∗27 confers risk for spondyloarthritis.Cell Chem Biol. 2025 Jan 16;32(1):12-24. doi: 10.1016/j.chembiol.2024.07.012. Epub 2024 Aug 20. Cell Chem Biol. 2025. PMID: 39168118 Review.
References
-
- Song I-H, Heldmann F, Rudwaleit M, Listing J, Appel H, Braun J, et al. . Different Response to Rituximab in Tumor Necrosis Factor Blocker-Naive Patients With Active Ankylosing Spondylitis and in Patients in Whom Tumor Necrosis Factor Blockers Have Failed: A Twenty-Four-Week Clinical Trial. Arthritis Rheum (2010) 62:1290–7. 10.1002/art.27383 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials