

Critical review of bone health, fracture risk and management of bone fragility in diabetes mellitus
- PMID: 34168723
- PMCID: PMC8192255
- DOI: 10.4239/wjd.v12.i6.706
Critical review of bone health, fracture risk and management of bone fragility in diabetes mellitus
Abstract
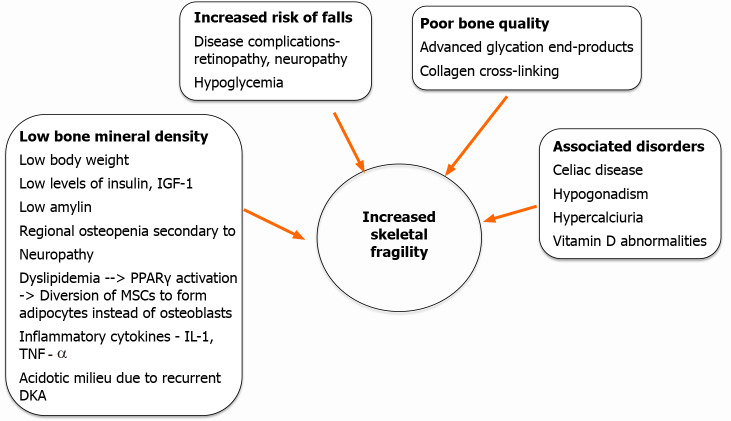
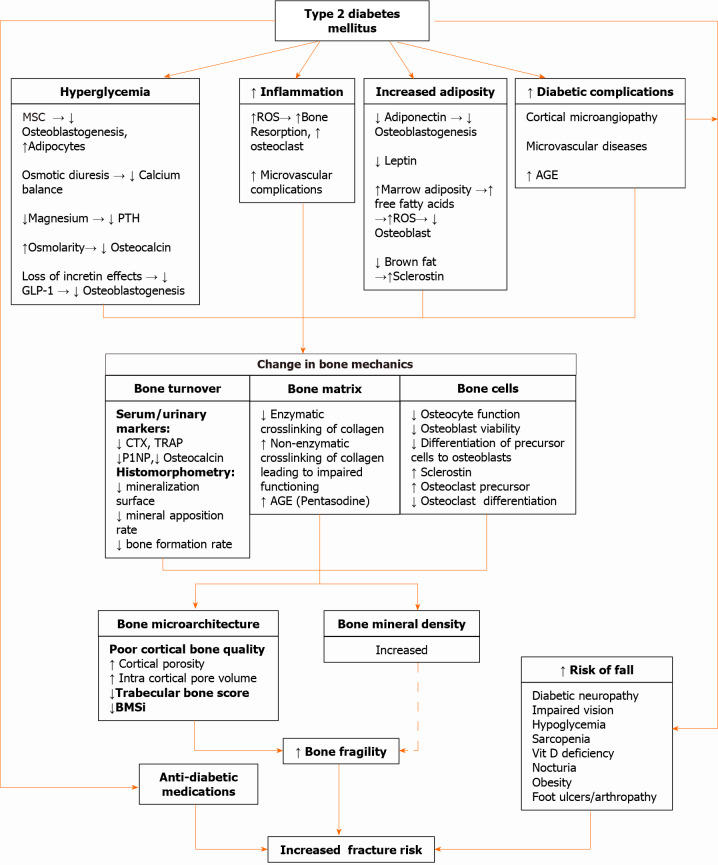
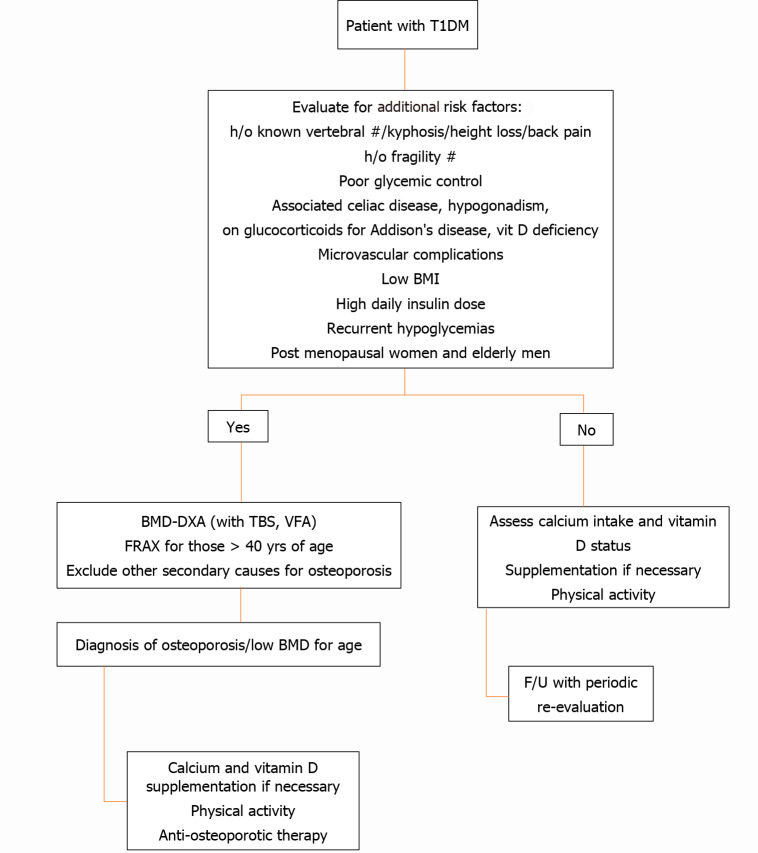
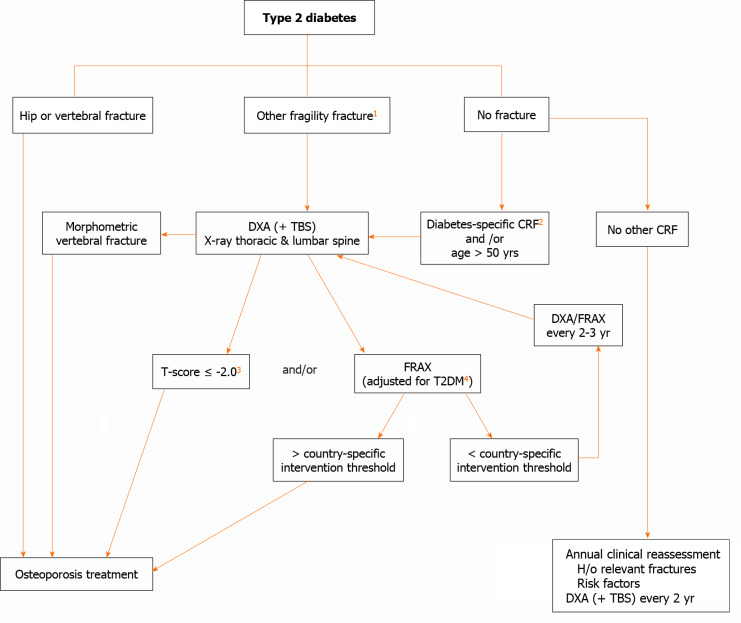
The risk of fracture is increased in both type 1 diabetes mellitus (T1DM) and type 2 diabetes mellitus (T2DM). However, in contrast to the former, patients with T2DM usually possess higher bone mineral density. Thus, there is a considerable difference in the pathophysiological basis of poor bone health between the two types of diabetes. Impaired bone strength due to poor bone microarchitecture and low bone turnover along with increased risk of fall are among the major factors behind elevated fracture risk. Moreover, some antidiabetic medications further enhance the fragility of the bone. On the other hand, antiosteoporosis medications can affect the glucose homeostasis in these patients. It is also difficult to predict the fracture risk in these patients because conventional tools such as bone mineral density and Fracture Risk Assessment Tool score assessment can underestimate the risk. Evidence-based recommendations for risk evaluation and management of poor bone health in diabetes are sparse in the literature. With the advancement in imaging technology, newer modalities are available to evaluate the bone quality and risk assessment in patients with diabetes. The purpose of this review is to explore the pathophysiology behind poor bone health in diabetic patients. Approach to the fracture risk evaluation in both T1DM and T2DM as well as the pragmatic use and efficacy of the available treatment options have been discussed in depth.
Keywords: Antidiabetic drugs; Antiosteoporosis therapy; Bone mineral density; Diabetes; Fracture risk; Microarchitecture.
©The Author(s) 2021. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: Nothing to disclose.
Figures
References
-
- International Diabetes Federation. IDF Diabetes Atlas 8th edition 2017. [cited 30 December 2020]. Available from: https://diabetesatlas.org/en/
-
- Napoli N, Chandran M, Pierroz DD, Abrahamsen B, Schwartz AV, Ferrari SL IOF Bone and Diabetes Working Group. Mechanisms of diabetes mellitus-induced bone fragility. Nat Rev Endocrinol. 2017;13:208–219. - PubMed
-
- Giangregorio LM, Leslie WD, Lix LM, Johansson H, Oden A, McCloskey E, Kanis JA. FRAX underestimates fracture risk in patients with diabetes. J Bone Miner Res. 2012;27:301–308. - PubMed
-
- Hofbauer LC, Brueck CC, Singh SK, Dobnig H. Osteoporosis in patients with diabetes mellitus. J Bone Miner Res. 2007;22:1317–1328. - PubMed
-
- Schwartz AV, Vittinghoff E, Bauer DC, Hillier TA, Strotmeyer ES, Ensrud KE, Donaldson MG, Cauley JA, Harris TB, Koster A, Womack CR, Palermo L, Black DM Study of Osteoporotic Fractures (SOF) Research Group; Osteoporotic Fractures in Men (MrOS) Research Group; Health; Aging and Body Composition (Health ABC) Research Group. Association of BMD and FRAX score with risk of fracture in older adults with type 2 diabetes. JAMA. 2011;305:2184–2192. - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
