

Droplet digital PCR-based detection of circulating tumor DNA from pediatric high grade and diffuse midline glioma patients
- PMID: 34169282
- PMCID: PMC8218704
- DOI: 10.1093/noajnl/vdab013
Droplet digital PCR-based detection of circulating tumor DNA from pediatric high grade and diffuse midline glioma patients
Abstract
Background: The use of liquid biopsy is of potential high importance for children with high grade (HGG) and diffuse midline gliomas (DMG), particularly where surgical procedures are limited, and invasive biopsy sampling not without risk. To date, however, the evidence that detection of cell-free DNA (cfDNA) or circulating tumor DNA (ctDNA) could provide useful information for these patients has been limited, or contradictory.
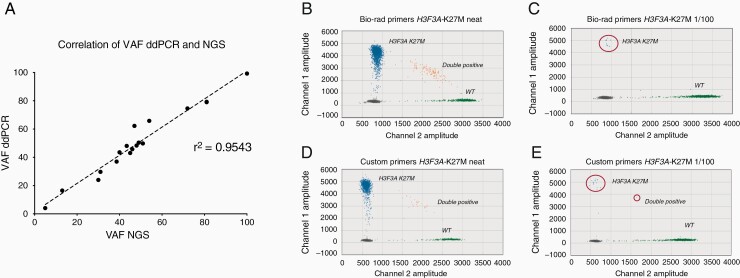
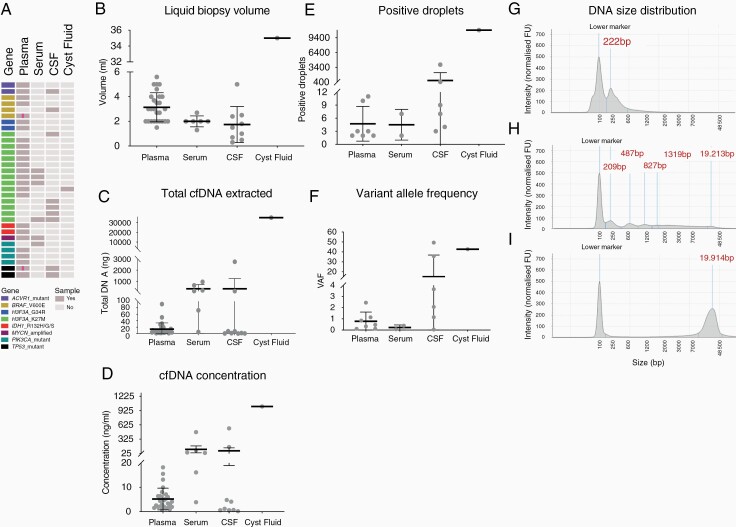
Methods: We optimized droplet digital PCR (ddPCR) assays for the detection of common somatic mutations observed in pediatric HGG/DMG, and applied them to liquid biopsies from plasma, serum, cerebrospinal fluid (CSF), and cystic fluid collected from 32 patients.
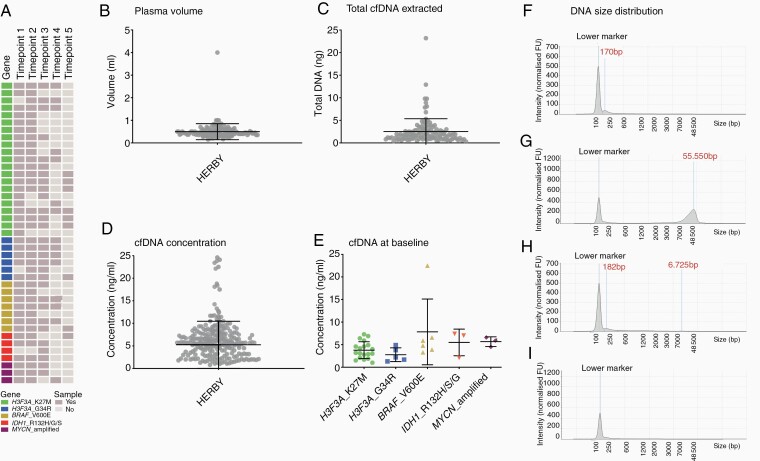
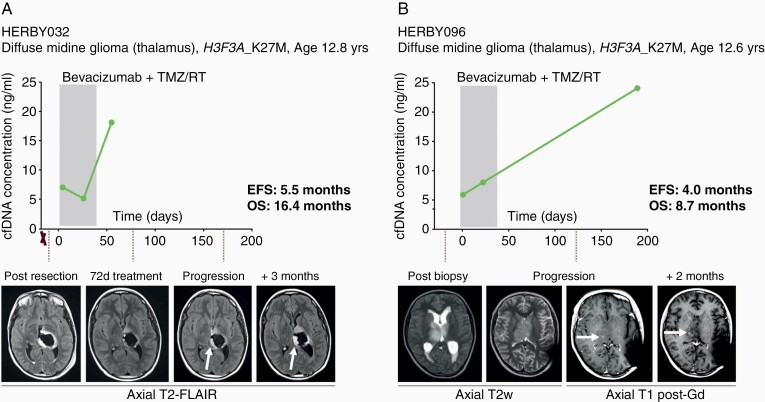
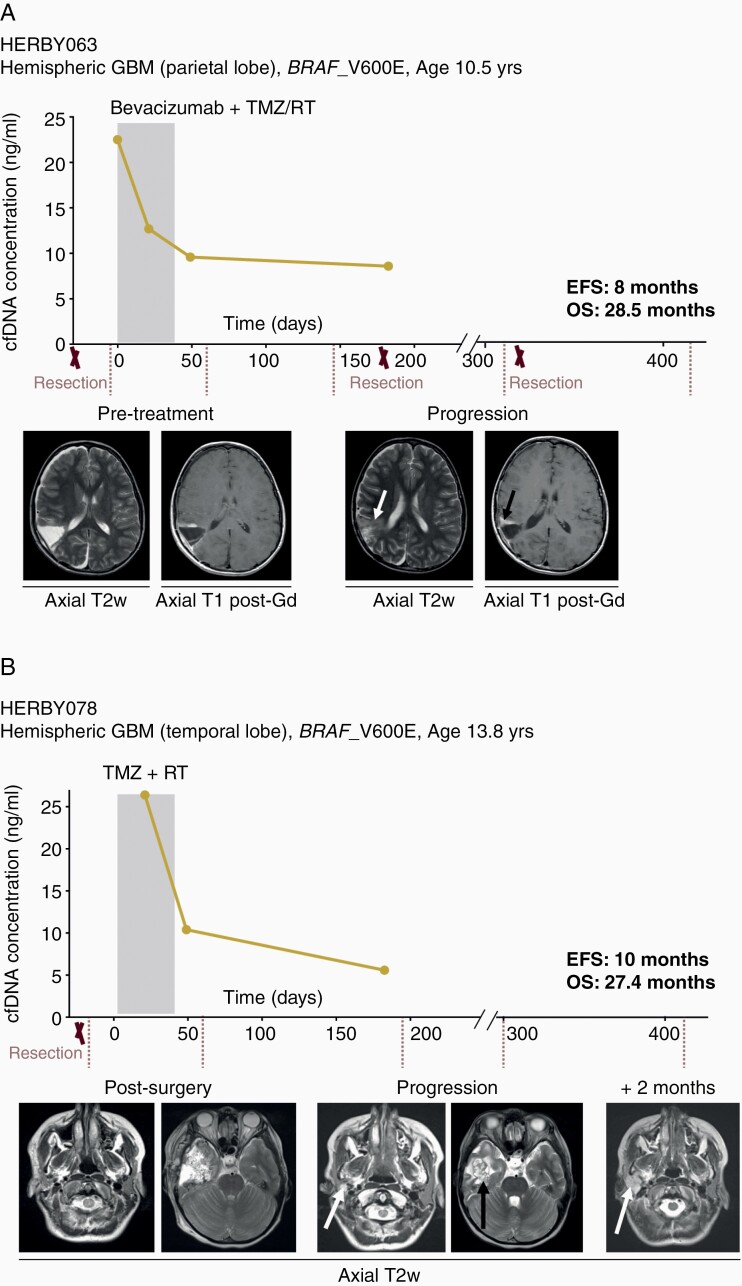
Results: Although detectable in all biomaterial types, ctDNA presented at significantly higher levels in CSF compared to plasma and/or serum. When applied to a cohort of 127 plasma specimens from 41 patients collected from 2011 to 2018 as part of a randomized clinical trial in pediatric non-brainstem HGG/DMG, ctDNA profiling by ddPCR was of limited use due to the small volumes (mean = 0.49 mL) available. In anecdotal cases where sufficient material was available, cfDNA concentration correlated with disease progression in two examples each of poor response in H3F3A_K27M-mutant DMG, and longer survival times in hemispheric BRAF_V600E-mutant cases.
Conclusion: Tumor-specific DNA alterations are more readily detected in CSF than plasma. Although we demonstrate the potential of the approach to assessing tumor burden, our results highlight the necessity for adequate sample collection and approach to improve detection if plasma samples are to be used.
Keywords: CSF; DIPG; HGG; cfDNA; ctDNA; plasma.
© The Author(s) 2021. Published by Oxford University Press, the Society for Neuro-Oncology and the European Association of Neuro-Oncology.
Figures
References
-
- Hamisch C, Kickingereder P, Fischer M, Simon T, Ruge MI. Update on the diagnostic value and safety of stereotactic biopsy for pediatric brainstem tumors: a systematic review and meta-analysis of 735 cases. J Neurosurg Pediatr. 2017;20(3):261–268. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials